Please cite this article as: CAO ZJ, GUO XG, SUN Q, CHEN YQ, XIE HY, YANG JD, WEI HQ, LI JH, MA J. Cryoballoon ablation of persistent atrial fibrillation for de novo pulmonary vein isolation: a single-center follow-up study. J Geriatr Cardiol 2022; 19(10): 725−733. DOI: 10.11909/j.issn.1671-5411.2022.10.001.
Citation:
Please cite this article as: CAO ZJ, GUO XG, SUN Q, CHEN YQ, XIE HY, YANG JD, WEI HQ, LI JH, MA J. Cryoballoon ablation of persistent atrial fibrillation for de novo pulmonary vein isolation: a single-center follow-up study. J Geriatr Cardiol 2022; 19(10): 725−733. DOI: 10.11909/j.issn.1671-5411.2022.10.001.
Please cite this article as: CAO ZJ, GUO XG, SUN Q, CHEN YQ, XIE HY, YANG JD, WEI HQ, LI JH, MA J. Cryoballoon ablation of persistent atrial fibrillation for de novo pulmonary vein isolation: a single-center follow-up study. J Geriatr Cardiol 2022; 19(10): 725−733. DOI: 10.11909/j.issn.1671-5411.2022.10.001.
Citation:
Please cite this article as: CAO ZJ, GUO XG, SUN Q, CHEN YQ, XIE HY, YANG JD, WEI HQ, LI JH, MA J. Cryoballoon ablation of persistent atrial fibrillation for de novo pulmonary vein isolation: a single-center follow-up study. J Geriatr Cardiol 2022; 19(10): 725−733. DOI: 10.11909/j.issn.1671-5411.2022.10.001.
Department of Cardiology, Sichuan Academy of Medical Sciences & Sichuan Provincial People’s Hospital, School of Medicine UESTC, Chengdu, China
2.
State Key Laboratory of Cardiovascular Disease, Arrhythmia Center, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China
3.
Department of Cardiology, Guangdong Cardiovascular Institute, Guangdong Provincial People’s Hospital, Guangdong Academy of Medical Science, Guangzhou, China
BACKGROUND Pulmonary vein isolation (PVI) alone for persistent atrial fibrillation (PersAF) remains controversial. The characteristics of cryoballoon ablation (CBA) to treat PersAF and the blanking period recurrence are underreported.
METHODS This study retrospectively analyzed patients with PersAF undergoing second-generation CBA for de novo PVI. The post-procedural efficacy and survival analysis were compared between patients with different PersAF durations. The multivariate Cox regression analysis was used to detect the risk factors for recurrence. Early and long-term recurrence were analyzed relative to each other.
RESULTS A total of 329 patients were enrolled, with a median PersAF duration of 4.0 months (interquartile range: 2.0–12.0 months); 257 patients (78.1%) were male. Kaplan-Meier analysis of freedom from atrial fibrillation recurrence at 12, 24, and 30 months showed 71.0%, 58.5%, and 54.9%, respectively. Early PersAF had a relatively favorable survival rate and a narrow P-wave duration of restoring sinus rhythm compared with that of PersAF lasting more than three months (P < 0.05). The multivariate Cox regression analysis revealed that PersAF duration and left atrial anteroposterior diameter ≥ 42 mm were the risk factors for atrial fibrillation recurrence after CBA [hazard ratio (HR) = 1.89, 95% CI: 1.01–1.4, P = 0.042; HR = 3.6, 95% CI: 2.4–5.4, P < 0.001, respectively]. The blanking period recurrence predicted the long-term recurrence (P < 0.0001).
CONCLUSIONS CBA of PersAF had safety and efficacy to reach de novo PVI. The PersAF duration and left atrial size were risk factors for atrial fibrillation recurrence after CBA. Blanking period recurrence was associated with long-term recurrence.
Persistent atrial fibrillation (PersAF) has been a long-held conundrum for rhythm control therapy due to the complex initiation and maintenance of atrial fibrillation (AF),[1] and the evidence-based efficacy of the catheter ablation of PersAF was superior to the medical therapies that reduce the AF burden or symptoms.[2,3] Currently, the cryoablation of PersAF has no uniform ablation strategy. Different ablation strategies for treating PersAF result in heterogeneous outcomes from its divergent pathogenesis. The empiric ablation of non-pulmonary vein foci or additional modification of the atrial substrate did not substantially improve the single procedural success rate or the recurrence.[4,5] Conversely, the incidence of procedure-related complications or atrial tachyarrhythmias may have increased.[6] Subsequently, the Substrate and Trigger Ablation for Reduction of Atrial Fibrillation Trial Part II (STAR AF II) study[7] further supported the cornerstone strategy of pulmonary vein isolation (PVI) for treating PersAF. In addition, early rhythm control therapy was associated with the reduction of adverse cardiovascular events.[8] Then, the latest evidence about cryoballoon ablation (CBA) of AF from the Cryoballoon Catheter Ablation in Antiarrhythmic Drug Naive Paroxysmal Atrial Fibrillation (STOP AF First) trial[9] and the Early Aggressive Invasive Intervention for Atrial Fibrillation (EARLY-AF) trial[10] restrictively enrolled patients with paroxysmal AF, but very little specific data have been identified for CBA in PersAF with different durations for de novo PVI.
This study was intended to evaluate the long-term efficacy of CBA of PersAF with different durations and to analyze the characteristics of blanking period recurrence with long-term recurrence.
METHODS
Study Population
Patients with PersAF undergoing CBA treatment for PVI from July 2016 to August 2018 in Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China were enrolled in this retrospective study. All patients had one or more symptoms to different degrees (i.e., palpitation, chest distress, shortness of breath or dyspnea, dizziness, fatigue, or physical limitations) and were refractory to at least one class I or class III antiarrhythmic drug. Blood specimens, transthoracic echocardiography, and computerized tomography confirmed the absence of structural and functional abnormalities (e.g., cardiomyopathy diseases, dilated left ventricle, pulmonary venous malformation, congenital heart diseases, and ejection fraction < 50%). Patients with any of the following items were excluded: history of surgery, prior radiofrequency ablation, age less than 18 years or more than 75 years. All patients provided written informed consent. This study was approved by the Institutional Review Board of Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China (No.2016-829). The guideline-based definitions of PersAF are as follows[1]: (1) PersAF is defined as continuous AF if it is sustained beyond seven days; (2) early PersAF (EPAF) is defined as PersAF lasting more than seven days but less than three months; and (3) long-standing PersAF (LSPAF) is defined as continuous PersAF lasting greater than 12 months.
Clinical Management of the Perioperative Period
All patients with PersAF received anticoagulant treatment more than three weeks before admission. After admission, all subjects took the therapeutic dose of amiodarone and a proton pump inhibitor. A value of the international normalized ratio was maintained, between 2.0 and 3.0. Left atrial thrombus was ruled out with transesophageal echocardiography before the procedure. Before the procedure, all antiarrhythmic drugs other than amiodarone were discontinued for a minimum of 5 half-lives and oral anticoagulants were discontinued for more than 24 h (except for warfarin). After discharge without contraindications, amiodarone and anticoagulants were prescribed to maintain the sinus rhythm and avoid thrombogenesis for three and two months, respectively. The proton pump inhibitor was continued for only two months. The subsequent rhythm control and anticoagulant strategy were at the discretion of physicians depending on the individual clinical manifestation and the CHA2DS2-VASc score.
Mapping Study and Cryoablation
The procedure-related electrocardiographic data were amplified and recorded on the Bard Electrophysiology recording system (LabSystem PRO; Bard Electrophysiology, Lowell, MA, USA). All vessel punctures used a local anesthesia strategy. A 6F decapolar electrode catheter was advanced into the coronary sinus via the right internal jugular vein or the subclavian vein. A 6F quadripolar electrode catheter was advanced into the right ventricular apex via the left femoral vein. The atrial transseptal maneuver was guided by fluoroscopy. Full-dose intravenous heparin (i.e., a dose of 100 IU/kg bolus) was administered upon left atrium access. The activated clotting time was assessed every 30 min to maintain a value of 300–350 s throughout the procedure.
Deep sedation was maintained with continuous intravenous fentanyl and midazolam. All real-time vital signs were under surveillance. A 12F steerable sheath (Arctic Front AdvanceTM, Medtronic, Minneapolis, MN, USA) was advanced into the left atrium via the right femoral vein. The cardiac cryoablation catheter (Arctic Front AdvanceTM, Medtronic, Minneapolis, MN, USA) was inserted into the manipulated sheath, and then the mapping catheter (Arctic Front AdvanceTM, Medtronic, Minneapolis, MN, USA) was advanced close to the ostium of the pulmonary vein via the inner lumen of the cryoballoon catheter. Contrast medium was injected to confirm the favorable occlusion and location of the cryoballoon upon inflation. The cryoablation protocol in our laboratory was as follows: (1) each freeze circle was set at 180 s; (2) once the time-to-isolation was more than 60 s or the cryotemperature within the first 60 s was higher than −40 °C, a second freeze cycle was necessary; (3) the nadir temperature of each freeze cycle was no lower than −60 °C; and (4) additional cryoapplications according to the individual’s condition was at the physicians’ discretion. Moreover, the backup right ventricular pacing or atropine were prepared to address the vagal reflex during the cryoablation of left-sided pulmonary veins, especially the left superior pulmonary veins (LSPVs); and the continuous phrenic nerve pacing (cycle length: 1500–2000 ms; high-output: 20 mA) was used to monitor potential phrenic palsy with tactile feedback on the patient’s abdomen during the cryoablation of right-sided pulmonary veins, especially the right superior pulmonary veins (RSPV). Importantly, cryoablation was terminated immediately upon the reduction or disappearance of phrenic stimulaton. The end point of cryoablation was PVI. In addition, the right atrial isthmus underwent linear ablation to achieve the bidirectional block to treat the typical atrial flutter (if electrocardiogram-documented atrial flutter was recorded before or during the procedure). Any cryoablation failure at the end of the procedure would undergo touch-up ablation with radiofrequency energy to achieve PVI.
Post-discharge Follow-up
All patients were scheduled for outpatient visits at one, two, and three months, and then every three months. The reexamination items included a 12-lead electrocardiography and 24-hour Holter monitoring. A telephone interview was initiated to confirm any meaningful self-reported symptoms. AF recurrence was defined as any documented atrial arrhythmia (i.e., atrial tachycardia or atrial flutter) episodes of more than 30 s. Freedom from recurrence was considered a procedural success, including in the survival analysis. All patients were expected to reach at least a two-year follow-up.
Statistical Analysis
Continuous variables are expressed as the mean ± SD or the median [interquartile range (IQR)], while categorical variables are described as counts (percentages). Kaplan-Meier was used to analyze the relationship between freedom from AF and survival time. A Cox proportional hazards model of univariate and multivariate risk factors was used to predict potential risk factors. Continuous variables were analyzed with parameter or non-parameter t-tests. Categorical variables were analyzed with the Pearson’s chi-squared test or Fisher’s exact probability test. Statistical analysis was analyzed with SPSS 20.0 (SPSS Inc., IBM, Chicago, IL, USA). The related figures were generated using GraphPad Prism 5.0 (GraphPad Software, San Diego, CA, USA). A P-value of < 0.05 was defined as statistically significant.
RESULTS
Baseline Participant Characteristics
A total of 329 patients with PersAF who were undergoing CBA were included, with a mean age of 50.3 ± 7.8 years and 257 patients (78.1%) being male. The median PersAF duration was 4.0 months (IQR: 2.0–12.0 months). The left atrial diameter, left ventricular end-diastolic diameter, and left ventricular ejection fraction were 42.0 ± 4.5 mm, 48.5 ± 4.0 mm, and 62.2% ± 4.2%, respectively. Before admission, 36 patients (10.9%) had histories of cerebral infarction or transient ischemic attack. Moreover, the age, AF duration, CHA2DS2-VASc scores, and P-wave duration of lead II during sinus rhythm among the baseline participants between the EPAF patients and patients with a PersAF duration more than three months showed significant statistical differences (P < 0.05) (Table 1).
Table
1.
Baseline participant characteristics.
Variables
Early PersAF (< 3 months)
Duration of PersAF (> 3 months)
P-value
n = 155
n = 174
Male
117 (75.5%)
140 (80.9%)
0.276
Age, yrs
56.7 ± 9.8
54.4 ± 9.2
0.029
Duration of atrial fibrillation, months
33.2 ± 50
46 ± 47.1
0.018
Body mass index, kg/m2
26.6 ± 3.6
26.5 ± 3.3
0.819
Left atrial diameter, mm
42.1 ± 4.5
41.9 ± 4.6
0.595
Left ventricular end-diastolic diameter, mm
48.4 ± 4.4
48.6 ± 3.7
0.614
Left ventricular ejection fraction, %
62.1 ± 4.4
62.3 ± 4.2
0.68
CHA2DS2-VASc scores
1.1 ± 1.1
1.4 ± 1.3
0.004
Hypertension
75 (48.4%)
77 (44.5%)
0.453
Coronary heart disease
22 (14.2%)
22 (12.7%)
0.881
Diabetes mellitus
15 (9.7%)
16 (9.2%)
0.746
Smoking
54 (34.8%)
71 (40.8%)
0.266
Hyperlipidemia
57 (36.8%)
51 (29.3%)
0.15
Stroke or transient ischemic attack
17 (11.0%)
19 (10.9%)
0.997
Bipolar P-wave
46 (29.7%)
50 (28.9%)
0.796
P-wave duration in lead II, ms
135.3 ± 22.6
140.8 ± 22.9
0.032
Brain natriuretic peptide, pg/mL
556.2 ± 584
576.5 ± 443.6
0.722
Data are presented as means ± SD or n (%). PersAF: persistent atrial fibrillation.
Unfortunately, 39 patients (11.9%) had acute single pulmonary vein cryoablation failure, accepting touch-up ablations using radiofrequency energy. The acute touch-up ablation sites were mostly localized, with sixteen cases of right inferior pulmonary veins, eight cases of LSPVs, six cases of left inferior pulmonary veins (LIPVs), one case of RSPV, six junctions of LSPV and LIPV, and two sites on the posterior atrial wall. In addition, 16 patients (14.5%) underwent cavotricuspid isthmus isolation with verification of the bidirectional conduction block. The mean procedure time was 54.6 ± 11.9 min with a mean X-ray exposure time of 17.7 ± 7.9 min and a dose of 257.9 ± 176.58 mGy.
Kaplan-Meier Survival Analysis
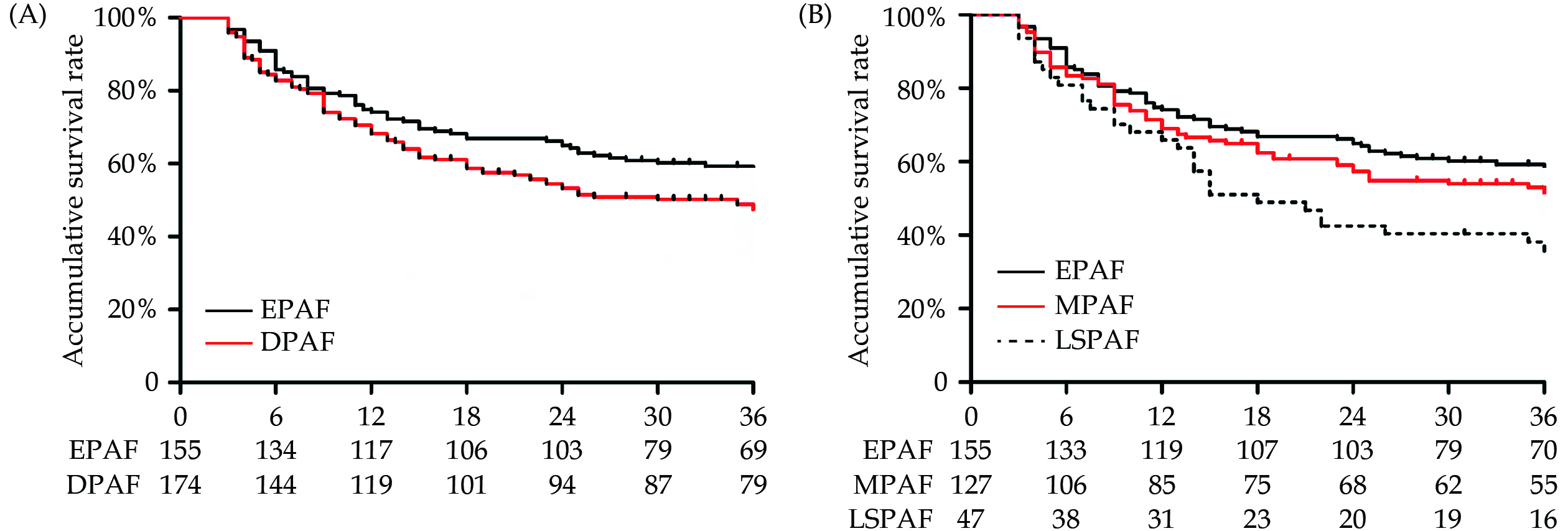
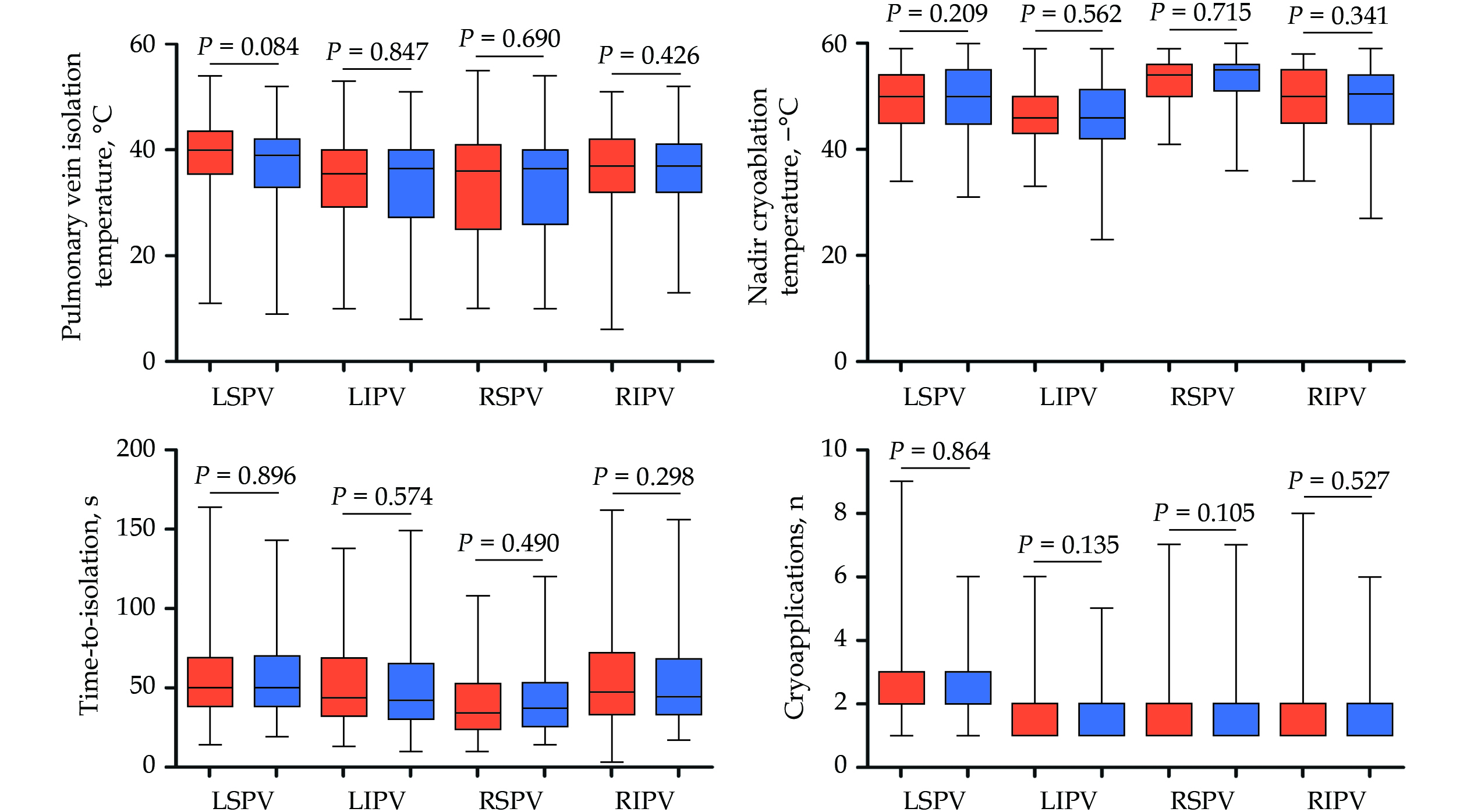
The median follow-up duration was 30.0 months (IQR: 10.0–43.0 months). Kaplan-Meier survival analysis showed that the cumulative survival rates of freedom from AF recurrence at 12, 24, and 30 months were 71.0%, 58.5%, and 54.9%, respectively. Analysis of the different disease courses of PersAF showed that the recurrence rate of AF after CBA in patients with EPAF was significantly lower than in those with PersAF lasting more than three months (P < 0.05). The cumulative survival rates of freedom from AF recurrence in patients with EPAF and LSPAF at 12, 24, and 30 months were 74.1%, 64.9%, and 60.2% versus 65.9%, 42.6% and 40.4%, respectively (P < 0.023) (Figure 1A). In addition, LSPAF patients had the lowest cumulative survival rate of freedom from AF recurrence compared with patients with a PersAF duration of fewer than 12 months (Figure 1B). Except for the form of AF recurrence showing as paroxysmal or PersAF, seven patients (4.3%) showed typical atrial flutter in combination with paroxysmal AF, two patients had atypical atrial flutter, and four patients had short episodes of atrial tachycardia. Furthermore, comparing time-to-isolation, PVI temperature, nadir cryoablation temperature, and the number of cryoablation applications between the AF recurrence and non-recurrence groups did not reveal significant statistical differences (P > 0.05) (Figure 2).
Figure
1.
The comparison of survival analysis.
(A): The atrial fibrillation relapse rate of EPAF was superior to that of DPAF; and (B): LSPAF had the highest atrial fibrillation relapse rate compared with the EPAF and MPAF. DPAF: duration of persistent atrial fibrillation; EPAF: early persistent atrial fibrillation; LSPAF: long-standing persistent atrial fibrillation; MPAF: middle persistent atrial fibrillation.
Figure
2.
The comparison of cryoablation parameters.
There were no significant statistical differences due to time-to-isolation, pulmonary vein isolation temperature, nadir cryoablation temperature, or the number of cryoablation applications between atrial fibrillation recurrence and non-recurrence. LIPV: left inferior pulmonary vein; LSPV: left superior pulmonary vein; RIPV: right inferior pulmonary vein; RSPV: right superior pulmonary vein.
Univariate and Multivariate Cox Regression Analysis
The univariate Cox regression analysis of hypertension, coronary heart disease, diabetes mellitus, left atrial anteroposterior diameter ≥ 42 mm, gender, age ≥ 60 years, inferior II lead with a bipolar P-wave, body mass index ≥ 26 kg/m2, and PersAF duration of more than three months showed that the duration of PersAF and left atrial anteroposterior diameter ≥ 42 mm were the risk factors for AF recurrence after CBA [hazard ratio (HR) = 1.89, 95% CI: 1.01–1.4, P = 0.042; HR = 3.6, 95% CI: 2.4–5.4, P < 0.001, respectively]. The multivariate Cox regression analysis also indicated that the duration of PersAF and left atrial anteroposterior diameter ≥ 42 mm were the risk factors for AF recurrence after CBA (HR = 3.64, 95% CI: 2.5–5.4, P < 0.001; HR = 1.38, 95% CI: 1.0–1.9, P = 0.043, respectively) (Table 2).
Table
2.
Univariate and multivariate Cox regression analysis.
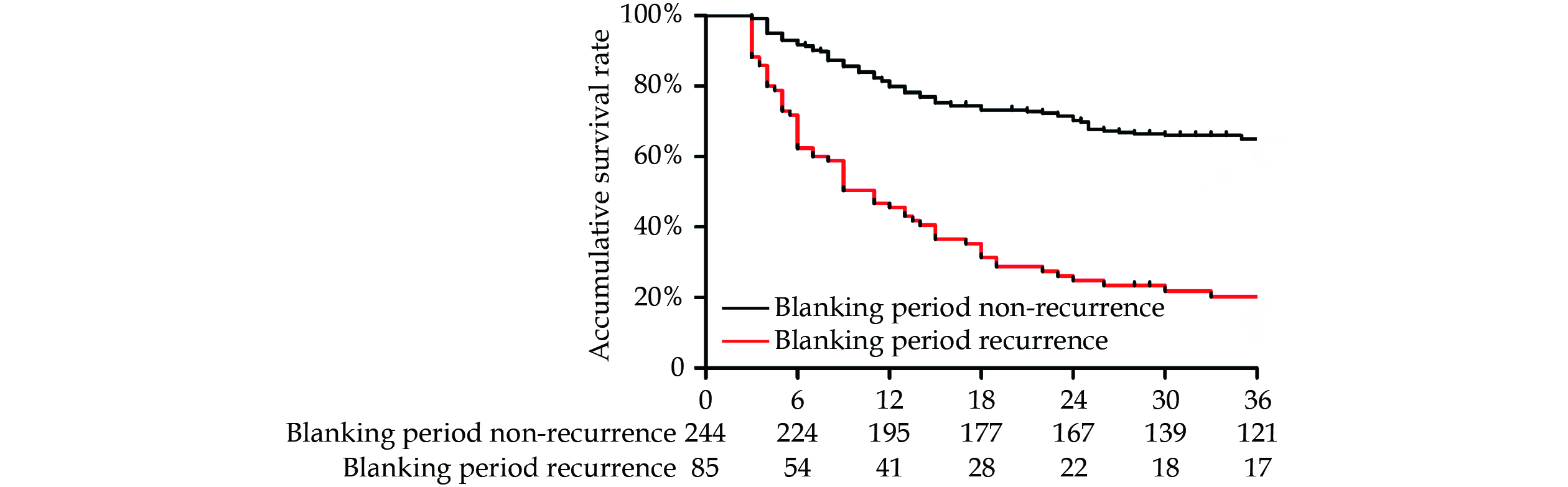
Overall, 85 patients (25.8%) had AF recurrence during the three-month blanking period. Kaplan-Meier survival analysis showed that the survival rates of freedom from recurrence at 12 and 30 months between the two groups with or without recurrence in the blanking period were 45.6% and 79.8%, and 21.9% and 66.0% (HR = 7.2, 95% CI: 4.7–10.9, P < 0.0001) (Figure 3). The AF recurrence in the three-month blanking period after CBA was suggestive of the long-term survival rate of freedom from AF, with a gradual reduction trend.
Figure
3.
The blanking period recurrence and survival analysis.
The long-term survival of patients with blanking period recurrence was remarkably lower.
Cryoablation of left-sided pulmonary veins induced 26 vagal reflexes (7.9%), including 24 cases of LSPV and two cases of LIPV. In total, 12 patients (3.6%) had acute transient phrenic paralysis during cryoablation of RSPV. No severe procedure-related complications occurred.
DISCUSSION
Main Findings
CBA of PersAF with different durations for de novo PVI was safe and effective, and a relatively long duration of PersAF and dilated left atrial as well as the potential electrical remodeling predicted the postprocedural AF recurrence. Additionally, AF recurrence during the blanking period was associated with long-term recurrence.
PersAF and PVI
Pulmonary vein foci were the major triggers for initiating AF,[11] and PVI was the cornerstone strategy for treating AF.[1] Moreover, the FIRE AND ICE trial has demonstrated that CBA is not inferior to radiofrequency ablation,[12] although the long-term prognosis outcomes of CBA for PersAF and de novo PVI alone are not clear, especially for PersAF with different durations. In 2015, Ciconte, et al.[13] reported a 12-month procedural success rate of 56% for second-generation CBA of PersAF. Thereafter, the follow-up success rate from the cryoablation of PersAF in different studies ranged from 67% to 86.8%.[14–16] Like the previously reported results, the 12-month follow-up success of this study was 71.0%. Additionally, this study enrolled patients with different durations of PersAF, and the prognosis result was close to the real-world outcomes focusing on the PVI alone of PersAF.
PersAF Duration and AF Recurrence
A pulmonary vein antrum isolation study showed that PersAF and LSPAF had relatively high rates of AF recurrence during the long-term follow-up.[17] The manifestation of PersAF was always suggestive of a relatively high AF burden, while the duration of PersAF was considered the risk factor for predicting AF recurrence. Kakuta, et al.[18] used a risk score model to assess AF recurrence after the Cryo-Maze procedure and found the duration of PersAF was associated with AF recurrence. In an observational study conducted by Takamiya, et al.,[19] a duration of PersAF greater than three years was associated with atrial tachyarrhythmia recurrence. The results of this study were consistent with the above-mentioned studies. A PersAF duration of more than three months resulted in a higher presentation of AF recurrence compared with EPAF patients, while patients with LSPAF had a markedly elevated incidence of AF recurrence during the long-term follow-up.
The progression of paroxysmal AF into PersAF is suggestive of the severity of atrial fibrosis and electrical remodeling.[20] Research data demonstrate the complex pathophysiology promoting the cellular matrix changes that disrupt the atrial cytoarchitecture,[21–23] mainly involving oxidative stress,[24] Ca2+-dependent intracellular processes,[25] atrial enlargement,[26] microRNA changes,[27] inflammation,[28] and myofibroblastic activation.[20] Hence, the deposition of extracellular matrix proteins generates the conduction disturbances[29] (i.e., the slow conduction, discontinuous conduction, and conduction blocks) becoming the culprits initiating and maintaining PersAF. Consistent with the presentation of atrial structural and electrical remodeling, the duration of the P-wave of inferior lead II after restoring the sinus rhythm in patients with EPAF was obviously shorter than that of patients with PersAF durations exceeding three months, especially in the LSPAF group. Therefore, the progression of PersAF is fundamentally accompanied by atrial substrate remodeling.[20,21,29]
Implications of Blanking Period Recurrence
Although blanking period recurrence is always considered an acute response to ablation,[1] the timing of AF recurrence clearly affects the long-term efficacy of CBA. Ciconte, et al.[13] found that atrial tachyarrhythmia occurrences during the blanking period seemed to be significant predictors of AF recurrence. The study about the pulmonary vein antrum isolation of PersAF demonstrated that the timing and frequency of early recurrences predicted long-term ablation success and was associated with the worse ablation success at one year,[17] while multiple early recurrences predicted long-term ablation failure more strongly than a single early recurrence. Like these two studies, this study found that patients with PersAF had a relatively high proportion of blanking period recurrences and that blanking period recurrence was associated with long-term recurrence. The published studies believed that not all early recurrence could be interpreted as transient inflammation or tissue necrosis and that early recurrence was likely an indirect marker of the severity of AF,[30] such as the advanced form of AF. In addition, early recurrence appearing as AF or macro-reentrant atrial tachycardia may represent the existing AF substrate supporting the mechanisms of perpetuation and maintenance.[1]
LIMITATIONS
There are several limitations that must be noted. Firstly, catheter ablation of PersAF lacks a uniform procedural strategy. Our study did not identify the specific mechanisms in the management of PersAF in individual patients that resulted in the single PVI strategy being insufficient, although the additional line ablation strategy in combination with PVI did not further enhance the success rate. Secondly, the majority of patients took only three-month supplies of amiodarone to maintain the sinus rhythm, which seemed insufficient to maintain a continuous serum concentration that would intervene in the abnormal electrical activities of the atrial myocardium. In addition, patients with asymptomatic AF were difficult to detect with one-time 24-hour Holter monitoring, while the implantable electrocardiogram monitoring device, as other studies have used, would have more signal acquisition to compensate for the shortage of outpatient visits. Last but not least, due to the limited number of patients with AF recurrence who underwent the redo procedure, the redo procedural information is not presented.
CONCLUSIONS
CBA safely and effectively treated PersAF. The duration of PersAF and the left atrial diameter were risk factors for AF recurrence after cryoablation. Blanking period recurrence was associated with long-term recurrence.
ACKNOWLEDGMENTS
This study was supported by the National Natural Science Foundation of China (No.81670309). All authors had no conflicts of interest to disclose.
Calkins H, Hindricks G, Cappato R, et al. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation. Europace 2018; 20: e1−e160. doi: 10.1093/europace/eux274
[2]
Poole JE, Bahnson TD, Monahan KH, et al. Recurrence of atrial fibrillation after catheter ablation or antiarrhythmic drug therapy in the CABANA trial. J Am Coll Cardiol 2020; 75: 3105−3118. doi: 10.1016/j.jacc.2020.04.065
[3]
Hunter RJ, Berriman TJ, Diab I, et al. A randomized controlled trial of catheter ablation versus medical treatment of atrial fibrillation in heart failure (the CAMTAF trial). Circ Arrhythm Electrophysiol 2014; 7: 31−38. doi: 10.1161/CIRCEP.113.000806
[4]
Fink T, Schlüter M, Heeger CH, et al. Stand-alone pulmonary vein isolation versus pulmonary vein isolation with additional substrate modification as index ablation procedures in patients with persistent and long-standing persistent atrial fibrillation: the randomized Alster-Lost-AF trial (Ablation at St. Georg Hospital for Long-Standing Persistent Atrial Fibrillation). Circ Arrhythm Electrophysiol 2017; 10: e005114. doi: 10.1161/CIRCEP.117.005114
[5]
Dixit S, Marchlinski FE, Lin D, et al. Randomized ablation strategies for the treatment of persistent atrial fibrillation: RASTA study. Circ Arrhythm Electrophysiol 2012; 5: 287−294. doi: 10.1161/CIRCEP.111.966226
[6]
Verma A, Sanders P, Champagne J, et al. Selective complex fractionated atrial electrograms targeting for atrial fibrillation study (SELECT AF): a multicenter, randomized trial. Circ Arrhythm Electrophysiol 2014; 7: 55−62. doi: 10.1161/CIRCEP.113.000890
[7]
Verma A, Jiang CY, Betts TR, et al. Approaches to catheter ablation for persistent atrial fibrillation. N Engl J Med 2015; 372: 1812−1822. doi: 10.1056/NEJMoa1408288
[8]
Kirchhof P, Camm AJ, Goette A, et al. Early rhythm-control therapy in patients with atrial fibrillation. N Engl J Med 2020; 383: 1305−1316. doi: 10.1056/NEJMoa2019422
[9]
Wazni OM, Dandamudi G, Sood N, et al. Cryoballoon ablation as initial therapy for atrial fibrillation. N Engl J Med 2021; 384: 316−324. doi: 10.1056/NEJMoa2029554
[10]
Andrade JG, Wells GA, Deyell MW, et al. Cryoablation or drug therapy for initial treatment of atrial fibrillation. N Engl J Med 2021; 384: 305−315. doi: 10.1056/NEJMoa2029980
[11]
Haïssaguerre M, Jaïs P, Shah DC, et al. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med 1998; 339: 659−666. doi: 10.1056/NEJM199809033391003
[12]
Kuck KH, Brugada J, Fürnkranz A, et al. Cryoballoon or radiofrequency ablation for paroxysmal atrial fibrillation. N Engl J Med 2016; 374: 2235−2245. doi: 10.1056/NEJMoa1602014
[13]
Ciconte G, Baltogiannis G, de Asmundis C, et al. Circumferential pulmonary vein isolation as index procedure for persistent atrial fibrillation: a comparison between radiofrequency catheter ablation and second-generation cryoballoon ablation. Europace 2015; 17: 559−565. doi: 10.1093/europace/euu350
[14]
Koektuerk B, Yorgun H, Hengeoez O, et al. Cryoballoon ablation for pulmonary vein isolation in patients with persistent atrial fibrillation: one-year outcome using second-generation cryoballoon. Circ Arrhythm Electrophysiol 2015; 8: 1073−1079. doi: 10.1161/CIRCEP.115.002776
[15]
Boveda S, Metzner A, Nguyen DQ, et al. Single-procedure outcomes and quality-of-life improvement 12 months post-cryoballoon ablation in persistent atrial fibrillation: results from the multicenter CRYO4PERSISTENT AF trial. JACC Clin Electrophysiol 2018; 4: 1440−1447. doi: 10.1016/j.jacep.2018.07.007
[16]
Su WW, Reddy VY, Bhasin K, et al. Cryoballoon ablation of pulmonary veins for persistent atrial fibrillation: results from the multicenter STOP Persistent AF trial. Heart Rhythm 2020; 17: 1841−1847. doi: 10.1016/j.hrthm.2020.06.020
[17]
Liang JJ, Elafros MA, Chik WW, et al. Early recurrence of atrial arrhythmias following pulmonary vein antral isolation: timing and frequency of early recurrences predicts long-term ablation success. Heart Rhythm 2015; 12: 2461−2468. doi: 10.1016/j.hrthm.2015.07.015
[18]
Kakuta T, Fukushima S, Minami K, et al. Novel risk score for predicting recurrence of atrial fibrillation after the Cryo-Maze procedure. Eur J Cardiothorac Surg 2021; 59: 1218−1225. doi: 10.1093/ejcts/ezaa468
[19]
Takamiya T, Nitta J, Inaba O, et al. Impact of diagnosis-to-ablation time on non-pulmonary vein triggers and ablation outcomes in persistent atrial fibrillation. J Cardiovasc Electrophysiol 2021; 32: 1251−1258. doi: 10.1111/jce.15002
[20]
Rohr S. Arrhythmogenic implications of fibroblast-myocyte interactions. Circ Arrhythm Electrophysiol 2012; 5: 442−452. doi: 10.1161/CIRCEP.110.957647
[21]
Jalife J, Kaur K. Atrial remodeling, fibrosis, and atrial fibrillation. Trends Cardiovasc Med 2015; 25: 475−484. doi: 10.1016/j.tcm.2014.12.015
[22]
Vasquez C, Mohandas P, Louie KL, et al. Enhanced fibroblast-myocyte interactions in response to cardiac injury. Circ Res 2010; 107: 1011−1020. doi: 10.1161/CIRCRESAHA.110.227421
[23]
Maesen B, Zeemering S, Afonso C, et al. Rearrangement of atrial bundle architecture and consequent changes in anisotropy of conduction constitute the 3-dimensional substrate for atrial fibrillation. Circ Arrhythm Electrophysiol 2013; 6: 967−975. doi: 10.1161/CIRCEP.113.000050
[24]
Kim YM, Kattach H, Ratnatunga C, et al. Association of atrial nicotinamide adenine dinucleotide phosphate oxidase activity with the development of atrial fibrillation after cardiac surgery. J Am Coll Cardiol 2008; 51: 68−74. doi: 10.1016/j.jacc.2007.07.085
[25]
Chiang DY, Kongchan N, Beavers DL, et al. Loss of microRNA-106b-25 cluster promotes atrial fibrillation by enhancing ryanodine receptor type-2 expression and calcium release. Circ Arrhythm Electrophysiol 2014; 7: 1214−1222. doi: 10.1161/CIRCEP.114.001973
[26]
Butt RP, Bishop JE. Mechanical load enhances the stimulatory effect of serum growth factors on cardiac fibroblast procollagen synthesis. J Mol Cell Cardiol 1997; 29: 1141−1151. doi: 10.1006/jmcc.1996.0347
[27]
Luo X, Yang B, Nattel S. MicroRNAs and atrial fibrillation: mechanisms and translational potential. Nat Rev Cardiol 2015; 12: 80−90. doi: 10.1038/nrcardio.2014.178
[28]
Guo Y, Lip GY, Apostolakis S. Inflammation in atrial fibrillation. J Am Coll Cardiol 2012; 60: 2263−2270. doi: 10.1016/j.jacc.2012.04.063
[29]
Nattel S, Heijman J, Zhou L, et al. Molecular basis of atrial fibrillation pathophysiology and therapy: a translational perspective. Circ Res 2020; 127: 51−72. doi: 10.1161/CIRCRESAHA.120.316363
[30]
Kim YG, Boo KY, Choi JI, et al. Early recurrence is reliable predictor of late recurrence after radiofrequency catheter ablation of atrial fibrillation. JACC Clin Electrophysiol 2021; 7: 343−351. doi: 10.1016/j.jacep.2020.09.029


 DownLoad:
DownLoad: