Please cite this article as: TU B, LAI ZH, CHEN AY, WENG ZY, CAI SM, ZHANG ZX, ZHOU LK, ZHENG LH, YAO Y. Effectiveness of cardioneuroablation in different subtypes of vasovagal syncope. J Geriatr Cardiol 2024; 21(6): 651−657. DOI: 10.26599/1671-5411.2024.06.004.
Citation:
Please cite this article as: TU B, LAI ZH, CHEN AY, WENG ZY, CAI SM, ZHANG ZX, ZHOU LK, ZHENG LH, YAO Y. Effectiveness of cardioneuroablation in different subtypes of vasovagal syncope. J Geriatr Cardiol 2024; 21(6): 651−657. DOI: 10.26599/1671-5411.2024.06.004.
Please cite this article as: TU B, LAI ZH, CHEN AY, WENG ZY, CAI SM, ZHANG ZX, ZHOU LK, ZHENG LH, YAO Y. Effectiveness of cardioneuroablation in different subtypes of vasovagal syncope. J Geriatr Cardiol 2024; 21(6): 651−657. DOI: 10.26599/1671-5411.2024.06.004.
Citation:
Please cite this article as: TU B, LAI ZH, CHEN AY, WENG ZY, CAI SM, ZHANG ZX, ZHOU LK, ZHENG LH, YAO Y. Effectiveness of cardioneuroablation in different subtypes of vasovagal syncope. J Geriatr Cardiol 2024; 21(6): 651−657. DOI: 10.26599/1671-5411.2024.06.004.
Arrhythmia Center, Fuwai Hospital, National Center for Cardiovascular Diseases, National Key Laboratory, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China
2.
Cardiac Center, Beijing Chaoyang Hospital, Capital Medical University, Beijing, China
3.
Cardiovascular Department, The First Affiliated Hospital, Fujian Medical University, Fujian Institute of Hypertension, Fujian, China
4.
Department of Cardiovascular, The Second Affiliated Hospital of Zhejiang University School of Medicine,Zhejiang, China
Cardioneuroablation (CNA) has shown encouraging results in patients with vasovagal syncope (VVS). However, data on different subtypes was scarce.
METHODS
This observational study retrospectively enrolled 141 patients [mean age: 40 ± 18 years, 51 males (36.2%)] with the diagnosis of VVS. The characteristics among different types of VVS and the outcomes after CNA were analyzed.
RESULTS
After a mean follow-up of 4.3 ± 1.5 years, 41 patients (29.1%) experienced syncope/pre-syncope events after CNA. Syncope/pre-syncope recurrence significantly differed in each subtype (P = 0.04). The cardioinhibitory type of VVS had the lowest recurrence rate after the procedure (n = 6, 16.7%), followed by mixed (n = 26, 30.6%) and vasodepressive (n = 9, 45.0%). Additionally, a significant difference was observed in the analyses of the Kaplan-Meier survival curve (P = 0.02). Syncope/pre-syncope burden was significantly reduced after CNA in the vasodepressive type (P < 0.01). Vasodepressive types with recurrent syncope/pre-syncope after CNA have a lower baseline deceleration capacity (DC) level than those without (7.4 ± 1.0 ms vs. 9.0 ± 1.6 ms, P = 0.01). Patients with DC < 8.4 ms had an 8.1 (HR = 8.1, 95% CI: 2.2–30.0, P = 0.02) times risk of syncope/pre-syncope recurrence after CNA compared to patients with DC ≥ 8.4 ms, and this association still existed after adjusting for age and sex (HR = 8.1, 95% CI: 2.2–30.1, P = 0.02).
CONCLUSIONS
Different subtypes exhibit different event-free rates. The vasodepressive type exhibited the lowest event-free rate, but those patients with DC ≥ 8.4 ms might benefit from CNA.
Nearly 40% of the population will experience at least one episode of syncope in their lifetime, and vasovagal syncope (VVS) is the most common cause.[1] Recurrent syncope episodes usually result in trauma and impaired quality of life. The impaired quality of life is close to diseases like chronic back pain, rheumatoid arthritis, and heart failure.[2–4] The incident rate of VVS peaks around 15-year-olds and 65-year-olds.[5] Related trauma caused by syncope spell anti-parallel with age, and nearly half of the elderly suffer from trauma compared to one-fourth in the youngsters.[6] Besides, severe incidents like fracture and concussion that lead by VVS also more prevail in the elderly.[6]
Treatment for VVS remains a challenge, while cardioneuroablation (CNA) shows encouraging results in preventing syncope/pre-syncope recurrence; however, the positive results were primarily reported in selected patients.[7–10] CNA merely ameliorates parasympathetic inhibition on cardio and does not directly affect sympathetic function on the vessel; hence the procedure might barely benefit patients of vasodepressive type logically.[11] Thus, most studies only include cardioinhibitory or mixed type for CNA.[7–10] The effectiveness of CNA on vasodepressive VVS remains undetermined, and the related data is limited. According to previous work, some positive results were also observed in vasodepressive type,[12–14] and this study aims to investigate the effectiveness of CNA in different types of VVS.
METHODS
Study Population
This observational study retrospectively enrolled 141 patients with VVS who underwent CNA from August 2015 to November 2021 in Fuwai Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China. Patients who met all the following criteria were included: (1) fulfilled the diagnostic criteria of VVS;[15] (2) underwent CNA that was only performed in the left atrium; (3) with a history of syncopal episodes more than three times and failed to treat with conventional therapy; and (4) with a positive response to the head-up tilt (HUT) test before CNA. Patients with the following conditions were excluded: (1) structural cardiac or cardiopulmonary diseases (cardiac valvular diseases, severe aortic stenosis, acute myocardial infarction within six months, pulmonary embolism, pulmonary hypertension, and hypertrophic obstructive cardiomyopathy); (2) cardiac arrhythmias that might lead to syncope (paroxysmal supraventricular tachycardia, ventricular tachycardia, and drug-induced arrhythmias); (3) cerebrovascular diseases (vascular steal syndromes and seizures); (4) medication-related syncope (vasodilators, anti-psychotics, and anti-diabetics); (5) condition that might affect the autonomic nerve (diabetes mellitus and nervous system–related diseases); and (6) terminal diseases or heart failure.
The Institutional Ethics Committee approved this study for Biomedical Research of Fuwai Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China. Written informed consent was obtained from all patients. The data supporting the findings of this study are available from the corresponding author upon reasonable request.
HUT Test
Patients were first undergoing a passive phase (tilted at 70° for 30 min), and an additional provocative phase (20 min with 0.25 mg sublingually administered nitroglycerin) was added when no positive results were induced during the passive phase. The detailed protocol of HUT test was described in the previous work from our center.[13,16,17] A positive response of HUT test was defined when syncope or pre-syncope occurs in the presence of bradycardia, hypotension, or both. The classification was based on the criteria proposed by VASIS (Vasovagal Syncope International Study).[18]
Deceleration Capacity (DC) Measurement
DC was obtained under the analyses of 24-hour electrocardiographic monitoring. The data were digitized at 128 Hz and automatically processed with specific software based on the phase-rectified signal averaging algorithm (MIC-12H Analysis Platform, Jinke Instruments, Beijing, China).[19,20] First, we set anchors at the heartbeat intervals longer than the preceding interval. To avoid errors caused by artifacts, R-R interval prolongations larger than 5% are excluded from the analysis process. Segments of the same size around the anchors are selected and aligned at the anchors. Then, signals X within the aligned segments are averaged. X0 and X1 are the averages of the anchor points and the following R-R intervals, and X-1 and X-2 are the averages of the 2 R-R intervals preceding the anchor points. DC is quantified using the following equation: DC = (1/4) (X0 + X1 – X-1 – X-2).
Process of CNA
The procedure has been described in our previous research.[13,14,17] Briefly, we used the EnSite NavX system (St. Jude Medical, Sao Paulo, Minnesota, USA) to guide the ganglion plexus (GP) ablation. Anatomical and high-frequency stimulation (HFS; 30 Hz, 20 V, pulse width 2 ms; MicroPace EPS320, Micropace EP, Sydney, Australia) were used to locate GPs. Once the 3-dimensional endocardial surface of the left atrium and pulmonary veins have been constructed, the sites of GPs can be first located by anatomy and then confirmed by HFS. A positive response of HFS was defined as transient ventricular asystole, atrioventricular block, or R-R interval increased by 50%. GP site could be anatomically located as follows: left superior GP (located in the superolateral area around the root of the left superior pulmonary vein); left inferior GP (located in the inferoposterior area around the root of the left inferior pulmonary vein); right anterior GP (located in the superoanterior area around the root of the right superior pulmonary vein), and right inferior GP (located in the inferoposterior area around the root of the right inferior pulmonary vein). GPs were ablated in the order of left superior GP–left inferior GP–right inferior GP–right anterior GP by a 4-mm tip radiofrequency ablation catheter once all the GPs had been located. Power and temperature were set with upper limits of 40 W and 60 °C, respectively. The endpoint of the ablation procedure was that HFS induced no vagal response.
Outcome and Follow-up
Routine follow-ups consisted of a clinical visit or contact by telephone every 6 months and carefully recorded related recurrence of syncope and pre-syncope.
Statistical Analysis
We performed the statistical analyses using the R statistical software 4.2 (R Foundation for Statistical Computing, Vienna, Austria). Continuous normally distributed, continuous nonnormally distributed and categorical variables were expressed as mean ± SD, median (interquartile range), and counts (percentages), respectively. We used the Pearson’s chi-squared test to compare the recurrence rate between the three groups. The Mann-Whitney U test was used to compare the syncope burden before and after the procedure. We performed logistic regression analyses to obtain the regression equation and then applied it to the receiver operating characteristic (ROC). The area under the curve was used to exhibit the discrimination value of DC. An optimal cut-off of DC was obtained at the maximum value of the sum of specificity and sensitivity through the ROC curve. Based on the optimal cut-off, DC was transformed into a dichotomous variable. Cox proportional hazard regression was used to calculate the associations between DC values and syncope/pre-syncope recurrence after ablation. Two-tailed P-value < 0.05 were considered statistically significant.
RESULTS
Baseline Characteristic
A total of 141 patients [mean age: 40 ± 18 years, 51 males (36.2%)] were included in this study, all with a positive result of HUT test. Mixed type (n = 85, 60.3%) was the most common type of VVS in our research, followed by cardioinhibitory (n = 36, 25.5%) and vasodepressive (n = 20, 14.2%). The baseline characteristics are shown in Table 1. The mean procedure time (skin to skin) was 128 ± 15 min. The mean total ablation time was 614 ± 142 s, and the mean total ablation site was 21 ± 5 sites. Inappropriate sinus tachycardia was observed in 10.6% (n = 15), and the patients were temporarily under medication (4 ivabradine, 11 beta-blockers). No complications, such as cardiac tamponade, cardiac rupture, left atrioesophageal fistula, peripheral vascular complications, etc., were observed.
Table
1.
Baseline characteristic.
Variables
Overall (n = 141)
Cardioinhibitory (n = 36)
Vasodepressive (n = 20)
Mixed (n = 85)
P-value
Age, yrs
40 ± 18
36 ± 16
46 ± 19
40 ± 18
0.11
Male
51 (36.2%)
18 (50%)
5 (25%)
28 (32.9%)
0.11
Body mass index, kg/m2
22.8 ± 3.5
23.0 ± 4.1
22.7 ± 3.6
22.7 ± 3.2
0.91
Systolic blood pressure, mmHg
121 ± 13
120 ± 13
120 ± 14
120 ± 13
0.99
Diastolic blood pressure, mmHg
71 ± 9
70 ± 8
71 ± 8
71 ± 10
0.76
Syncope burden
Disease duration, yrs
3 (1–11)*
2 (0.9–6)*
2.5 (0.5–12)*
3.5 (2–13)*
0.11
1-year burden, times
2 (1–4)*
2 (1–3)*
3 (2–4)*
2 (1–4)*
0.18
24-hour electrocardiogram monitor
Mean heart rate, beats/min
69 ± 11
66 ± 14
69 ± 10
70 ± 9
0.26
Standard deviation of all average normal-to- normal intervals, ms
147 ± 51
163 ± 69
138 ± 31
140 ± 42
0.08
Root mean square of the successive differences of all normal-to-normal intervals, ms
43 (32–55)*
44 (33–59)*
42 (30–48)*
42 (31–56)*
0.19
Triangle index, ms
39 ± 10
39 ± 8
35 ± 10
39 ± 12
0.49
High frequency normalized, ms2
36 ± 10
34 ± 12
37 ± 9
37 ± 9
0.08
Low frequency normalized, ms2
48 ± 12
51 ± 12
41 ± 14
47 ± 12
0.09
Very low frequency, ms2
703 (492–1052)*
866 (588–1287)*
342 (277–756)*
680 (132–423)*
0.03
Low frequency/High frequency
1.59 (1.29–2.34)*
1.87 (1.20–2.81)*
1.50 (0.88–1.64)*
1.58 (1.32–2.15)*
0.20
Deceleration capacity, ms
10.4 ± 3.9
11.4 ± 4.6
8.2 ± 2.5
10.7 ± 3.8
0.01
Acceleration capacity, ms
10.1 ± 3.7
10.8 ± 4.4
8.1 ± 1.5
10.3 ± 3.6
0.02
General therapy
Nonpharmacologic
141 (100%)
36 (100%)
20 (100%)
85 (100%)
Beta-blocker
6 (4.3%)
0
2 (10%)
4 (4.7%)
0.17
Midodrine
9 (6.3%)
1 (2.8%)
5 (25%)
3 (3.5%)
0.01
Fludrocortisone
2 (1.4%)
0
1 (5%)
1 (1.1%)
0.33
Data are presented as means ± SD or n (%). *Presented as median (interquartile range).
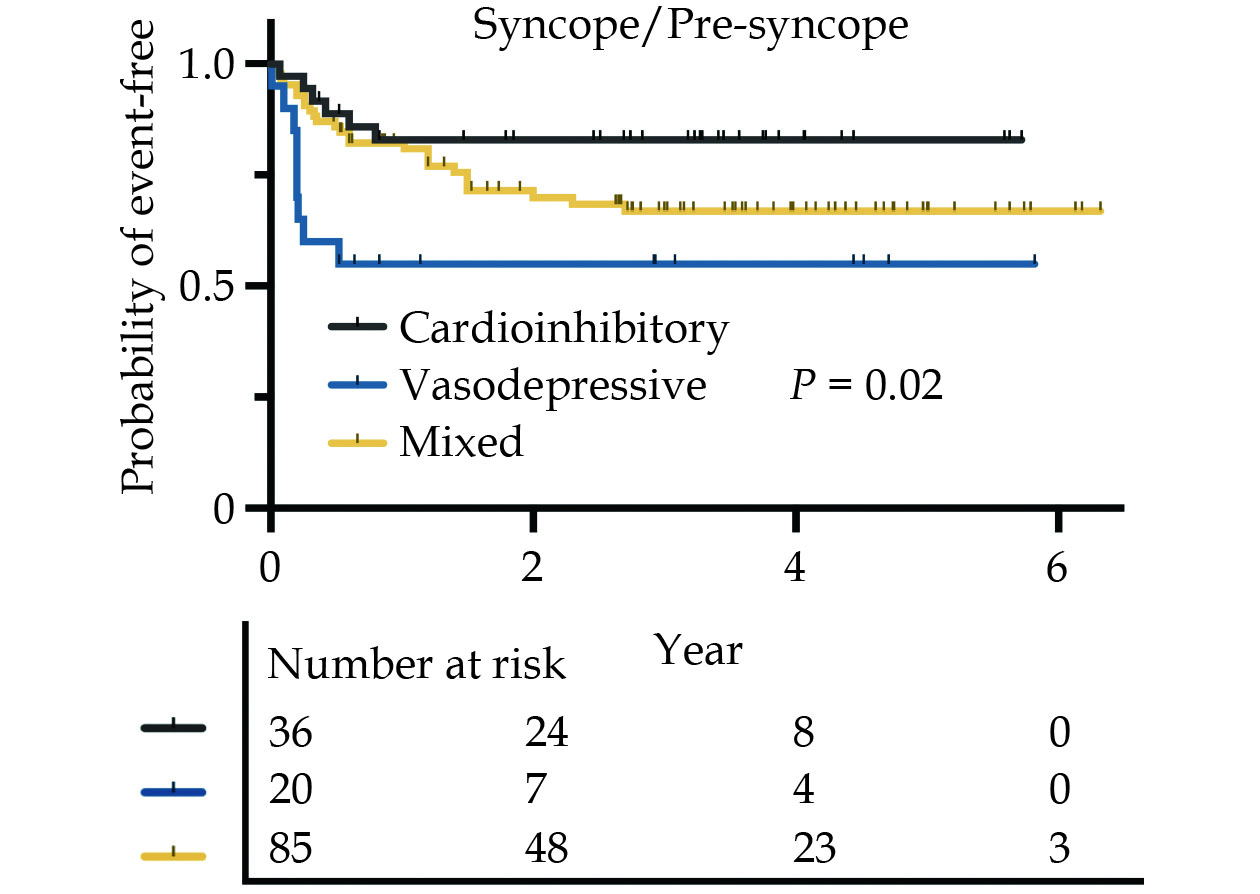
With a mean follow-up time of 4.3 ± 1.5 years, 41 patients (29.1%) recorded at least one episode of syncope/pre-syncope events, and nine patients (6.3%) only experienced pre-syncope events. Syncope/pre-syncope recurrence significantly differed in each subtype (P = 0.04). The cardioinhibitory type of VVS had the lowest recurrence rate after the procedure (n = 6, 16.7%), followed by mixed (n = 26, 30.6%) and vasodepressive type (n = 9, 45.0%). Additionally, a significant difference in syncope/pre-syncope recurrence was observed among different types of VVS in the analyses of the Kaplan-Meier survival curve (P = 0.02, Figure 1). Out of all the patients, 16 patients (11.3%) were over 65 years old and had a recurrence rate of 31.2% (n = 5), while those under 65 years old (n = 125) had a recurrence rate of 28.8% (n = 36). The difference between the two groups was not statistically significant according to the Pearson’s chi-squared test (P = 0.582).
Figure
1.
The Kaplan-Meier survival curve for syncope/pre-syncope recurrence.
Syncope/Pre-syncope Recurrence in Vasodepressive Type of VVS
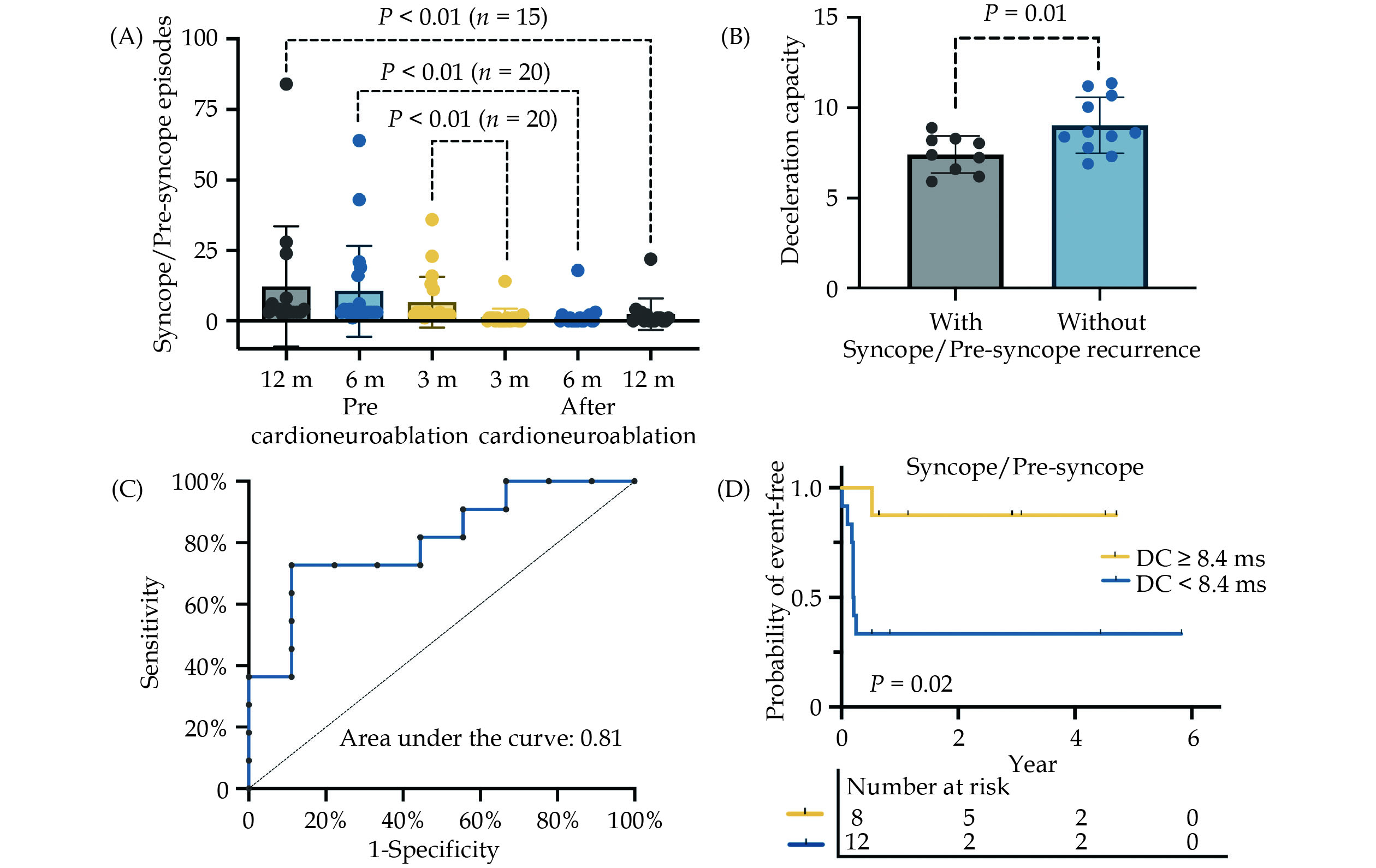
Twenty patients (14.2%) with vasodepressive VVS underwent CNA in this study, and nearly half of them (45.0%, n = 9) recorded recurrent syncope/pre-syncope events. The median (interquartile range) syncope burden before the procedure was 2 (1.3–3), 2 (2–4), 2 (2–4) in 3 months, 6 months, and 12 months separately. The median (interquartile range) syncope burden after the procedure was 0.5 (0.5–1), 0.5 (0.5–1), 0.5 (0.5–1) in 3 months, 6 months, and 12 months separately. A significant reduction was observed in syncope/pre-syncope burden after CNA (P < 0.01) as shown in Figure 2A. Compared to the event-free ones (Figure 2B), recurrent patients were associated with a lower level of DC (9.0 ± 1.6 ms vs. 7.4 ± 1.0 ms, P = 0.01). Results of the comparison between recurrent and event-free ones were summarized in Table 2. In the analyses of the ROC curve (Figure 2C), DC showed a discrimination value of 0.81 for predicting syncope/pre-syncope recurrence. The optimal cut-off of DC was set at 8.4 ms, with a sensitivity of 0.73 and specificity of 0.89. Patients with DC < 8.4 ms had an 8.1 (HR = 8.1, 95% CI: 2.2–30.0, P = 0.02) times the risk of syncope/pre-syncope recurrence after CNA (Figure 2D), and this effect still existed after adjusting for age and sex (HR = 8.1, 95% CI: 2.2–30.1, P = 0.02).
Figure
2.
Effectiveness of cardioneuroablation in patients with vasovagal syncope vassodepressive and the predictive values DC.
(A): The median (interquartile range) syncope burden before the procedure was 2 (1.3–3), 2 (2–4), 2 (2–4) in 3 months, 6 months, and 12 months separately. The median (interquartile range) syncope burden after the procedure was 0.5 (0.5–1), 0.5 (0.5–1), 0.5 (0.5–1) in 3 months, 6 months, and 12 months separately. A significant reduction was observed in syncope/pre-syncope burden after cardioneuroablation in the vasodepressive type of vasovagal syncope, and the P-values were carried out by the Mann-Whitney U test; (B): compared to the recurrent ones, patients without syncope/pre-syncope recurrence showed a lower DC level with statistical significance (P = 0.01) by using the Student’s t-test; (C): DC showed an area under the curve of 0.81 for discrimination values of syncope/pre-syncope recurrence. The optimal cut-off was set at 8.4 ms with a sensitivity of 0.73 and specificity of 0.89; and (D): patients with DC < 8.4 ms had an 8.1 times risk of syncope/pre-syncope recurrence after cardioneuroablation compared to patients with DC ≥ 8.4 ms (P = 0.02), HR was obtained with Cox proportional hazard regression. DC: deceleration capacity.
Various studies demonstrate that CNA is a promising therapy for patients with VVS, while the effectiveness among different types of VVS has yet to be specifically discussed. The efficacy of CNA was significantly different in each subtype of VVS, while no significant difference in efficacy was observed with age. CNA denervated the cardiac through the damage of GPs, which mainly contains the soma of parasympathetic neuron,[21] compatible with the fact that a significant increase in heart rate was observed after the procedure. Logically, CNA merely weakens cardiac parasympathetic tension and does not directly affect the modulation of sympathetic nerves on vessels. Hence, significant differences in event-free rate were observed among different types of VVS, and the vasodepressive VVS exhibited the lowest event-free rate. Patients with mixed type transformed into vasodepressive type after CNA also implied that the procedures merely alleviated the cardioinhibition.[22] However, 55% of patients showed no syncope/pre-syncope recurrence after CNA in vasodepressive VVS, and the syncope/pre-syncope burden was significantly reduced after the procedure might provide that CNA might benefit vasodepressive type. A few hypotheses also suggested that CNA might benefit vasodepressive types but needed further confirmation. A significant elevation in heart rate was observed after CNA in this study and other studies.[7,14] The elevated heart rate might compensate for the vasodilation during the syncope episode. Additionally, CNA might alleviate vasodepression through afferent nerve denervation. Baroreflex dysfunction was proposed as a mechanism in VVS,[23] and CNA impaired both the efferent and afferent nerve of the baroreflex in the heart. The damaged cardiac efferent nerve merely alleviates the cardioinhibition. Still, the impaired afferent nerve might reduce the activity of the efferent nerve, which functions on both cardio and vessels.
From previous study,[12] DC showed discrimination values for distinguishing syncope/pre-syncope recurrence after CNA; patients with higher baseline DC levels were more likely to benefit from the procedure. Besides, multiple studies suggested that DC reflects the cardiac parasympathetic nerve tension.[19,24] Consistent with previous results, a gradual declination of DC was observed in cardioinhibitory, mixed, and vasodepressive. Besides, the vasodepressive exhibited the lowest DC level and lowest success rate in this study reconfirmed previous results. Considering the low reproducibility of HUT, the partial vasodepressive type might be misclassified. A DC value exceeding 8.4 ms might represent a relatively high level of parasympathetic tension in vasodepressive types and generate a more beneficial result after CNA.
However, the relatively positive results might be explained with the following hypotheses. First, HUT might be insufficient to separate different types of VVS accurately. Patients with other types of VVS might be misclassified into vasodepressive types. HUT shows unpleasant reproducibility ranging from 31% to 92%,[25–27] and several studies have reported discordant classification between sequential HUT.[28] Second, the overall positive results might originate from the placebo effect, considering the placebo effect may account for over half of the clinical effect.[29] Studies show that a reduced risk of syncope recurrence was witnessed in over half of the patients through pure clinical visits.[1]
LIMITATIONS
The retrospective nature of the study limited the interpretation of the results; hence, the implications of this study should instead be interpreted as an insight to encourage the application of CNA on vasodepressive type. Another major limitation was that there was no control group in this study. Further randomized control trials needed to be carried out to confirm those results.
CONCLUSIONS
CNA effectively reduced syncope/presyncope recurrence in patients with VVS; however, a significant difference in recurrence rate was observed in different subtypes. The vasodepressive type exhibited the lowest event-free rate, but those patients with DC ≥ 8.4 ms might benefit from CNA.
ACKNOWLEDGMENTS
This study was supported by the CAMS Central Public Welfare Scientific Research Institute Basal Research Expenses (No.2021-XCGC09-1 & No.2022-I2M-C&T-B-045), the Beijing Municipal Science & Technology Commission (Z191100006619019), and the High-level Hospital Clinical Scientific Research Business Fees (No.2022-GSP-QZ-4). All authors had no conflicts of interest to disclose.
Shen WK, Sheldon RS, Benditt DG, et al. 2017 ACC/AHA/HRS guideline for the evaluation and management of patients with syncope: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. He art Rhythm 2017; 14: e155−e217. doi: 10.1016/j.hrthm.2017.03.004
[2]
Rose MS, Koshman ML, Spreng S, et al. The relationship between health-related quality of life and frequency of spells in patients with syncope. J Clin Epidemiol 2000; 53: 1209−1216. doi: 10.1016/S0895-4356(00)00257-2
[3]
Gong J, Ding Y, Wang J, et al. Insufficiency of quality of life as the treatment endpoint for balloon pulmonary angioplasty in inoperable chronic thromboembolic pulmonary hypertension. J Transl Int Med 2024; 12: 148−156. doi: 10.2478/jtim-2022-0067
[4]
Ng J, Sheldon RS, Ritchie D, et al. Reduced quality of life and greater psychological distress in vasovagal syncope patients compared to healthy individuals. Pacing Clin Electrophysiol 2019; 42: 180−188. doi: 10.1111/pace.13559
[5]
Sheldon RS, Sheldon AG, Connolly SJ, et al. Age of first faint in patients with vasovagal syncope. J Cardiovasc Ele ctrophysiol 2006; 17: 49−54. doi: 10.1111/j.1540-8167.2005.00267.x
[6]
Jorge JG, Raj SR, Teixeira PS, et al. Likelihood of injury due to vasovagal syncope: a systematic review and meta-analysis. Europace 2021; 23: 1092−1099. doi: 10.1093/europace/euab041
[7]
Debruyne P, Rossenbacker T, Janssens L, et al. Durable physiological changes and decreased syncope burden 12 months after unifocal right-sided ablation under computed tomographic guidance in patients with neurally mediated syncope or functional sinus node dysfunction. Circ Arrhythm Electrophysiol 2021; 14: e009747. doi: 10.1161/CIRCEP.120.009747
[8]
Aksu T, Guler TE, Bozyel S, et al. Medium-term results of cardioneuroablation for clinical bradyarrhythmias and vasovagal syncope: effects on QT interval and heart rate. J Interv Card Electrophysiol 2021; 60: 57−68. doi: 10.1007/s10840-020-00704-2
[9]
Pachon JC, Pachon EI, Cunha Pachon MZ, et al. Catheter ablation of severe neurally meditated reflex (neurocardiogenic or vasovagal) syncope: cardioneuroablation long-term results. Europace 2011; 13: 1231−1242. doi: 10.1093/europace/eur163
[10]
Pachon M JC, Pachon M EI, Santillana P TG, et al. Simplified method for vagal effect evaluation in cardiac ablation and electrophysiological procedures. JACC Clin Electrop hysiol 2015; 1: 451−460. doi: 10.1016/j.jacep.2015.06.008
[11]
Sutton R. Should we treat severe vasovagal syncope with a pacemaker? J Intern Med 2017; 281: 554–561.
[12]
Tu B, Wu L, Hu F, et al. Cardiac deceleration capacity as an indicator for cardioneuroablation in patients with refractory vasovagal syncope. Heart Rhythm 2022; 19: 562−569. doi: 10.1016/j.hrthm.2021.12.007
[13]
Sun W, Zheng L, Qiao Y, et al. Catheter ablation as a treatment for vasovagal syncope: long-term outcome of endocardial autonomic modification of the left atrium. J Am He art Assoc 2016; 5: e003471. doi: 10.1161/JAHA.116.003471
[14]
Hu F, Zheng L, Liang E, et al. Right anterior ganglionated plexus: the primary target of cardioneuroablation? Heart Rhythm 2019; 16: 1545–1551.
[15]
Sheldon RS, Grubb BP 2nd, Olshansky B, et al. 2015 Heart Rhythm Society expert consensus statement on the diagnosis and treatment of postural tachycardia syndrome, inappropriate sinus tachycardia, and vasovagal syncope. Hea rt Rhythm 2015; 12: e41−e63. doi: 10.1016/j.hrthm.2015.03.029
[16]
Zheng L, Sun W, Liu S, et al. The diagnostic value of cardiac deceleration capacity in vasovagal syncope. Circ Arr hythm Electrophysiol 2020; 13: e008659. doi: 10.1161/CIRCEP.120.008659
[17]
Yao Y, Shi R, Wong T, et al. Endocardial autonomic denervation of the left atrium to treat vasovagal syncope: an early experience in humans. Circ Arrhythm Electrophysiol 2012; 5: 279−286. doi: 10.1161/CIRCEP.111.966465
[18]
Sutton R, Brignole M, Menozzi C, et al. Dual-chamber pacing in the treatment of neurally mediated tilt-positive cardioinhibitory syncope: pacemaker versus no therapy: a multicenter randomized study. The Vasovagal Syncope International Study (VASIS) Investigators. Circulation 2000; 102: 294−299.
[19]
Xu Y, Wan W, Zeng H, et al. Exosomes and their derivatives as biomarkers and therapeutic delivery agents for cardiovascular diseases: situations and challenges. J Transl Int Med 2023; 11: 341−354. doi: 10.2478/jtim-2023-0124
[20]
Carricarte Naranjo C, Marras C, Visanji NP, et al. Short-term deceleration capacity of heart rate: a sensitive marker of cardiac autonomic dysfunction in idiopathic Parkinson’s disease. Clin Auton Res 2021; 31: 729−736. doi: 10.1007/s10286-021-00815-4
[21]
Pachon-M JC, Pachon-M EI, Pachon CTC, et al. Long-term evaluation of the vagal denervation by cardioneuroablation using Holter and heart rate variability. Circ Arrhythm Electrophysiol 2020; 13: e008703. doi: 10.1161/CIRCEP.120.008703
[22]
Aksu T, Guler TE, Bozyel S, et al. Usefulness of post-procedural heart rate response to predict syncope recurrence or positive head up tilt table testing after cardioneuroablation. Europace 2020; 22: 1320−1327. doi: 10.1093/europace/euaa230
[23]
Kaufmann H, Norcliffe-Kaufmann L, Palma JA. Baroreflex dysfunction. N Engl J Med 2020; 382: 163−178. doi: 10.1056/NEJMra1509723
[24]
Duckheim M, Gaebler M, Mizera L, et al. Deceleration capacity for rapid risk stratification in patients suffering from acute ischemic stroke: a prospective exploratory pilot study. Medicine (Baltimore) 2021; 100: e25333. doi: 10.1097/MD.0000000000025333
[25]
Fitzpatrick AP, Theodorakis G, Vardas P, et al. Methodology of head-up tilt testing in patients with unexplained syncope. J Am Coll Cardiol 1991; 17: 125−130. doi: 10.1016/0735-1097(91)90714-K
[26]
Aponte-Becerra L, Novak P. Tilt test: a review. J Clin Ne urophysiol 2021; 38: 279−286. doi: 10.1097/WNP.0000000000000625
[27]
Brignole M, Moya A, de Lange FJ, et al. 2018 ESC guidelines for the diagnosis and management of syncope. Eur He art J 2018; 39: 1883−1948. doi: 10.1093/eurheartj/ehy037
[28]
Brignole M, Sutton R, Menozzi C, et al. Lack of correlation between the responses to tilt testing and adenosine triphosphate test and the mechanism of spontaneous neurally mediated syncope. Eur Heart J 2006; 27: 2232−2239. doi: 10.1093/eurheartj/ehl164
[29]
Sheldon R, Opie-Moran M. The placebo effect in cardiology: understanding and using it. Can J Cardiol 2017; 33: 1535−1542. doi: 10.1016/j.cjca.2017.09.017


 DownLoad:
DownLoad: