Please cite this article as: LI M, WEI N, SHI HY, JING XJ, KAN XH, GAO HQ, XIAO YL. Prevalence and clinical implications of polypharmacy and potentially inappropriate medication in elderly patients with heart failure: results of six months' follow-up. J Geriatr Cardiol 2023; 20(7): 495−508. DOI: 10.26599/1671-5411.2023.07.002.
Citation:
Please cite this article as: LI M, WEI N, SHI HY, JING XJ, KAN XH, GAO HQ, XIAO YL. Prevalence and clinical implications of polypharmacy and potentially inappropriate medication in elderly patients with heart failure: results of six months' follow-up. J Geriatr Cardiol 2023; 20(7): 495−508. DOI: 10.26599/1671-5411.2023.07.002.
Please cite this article as: LI M, WEI N, SHI HY, JING XJ, KAN XH, GAO HQ, XIAO YL. Prevalence and clinical implications of polypharmacy and potentially inappropriate medication in elderly patients with heart failure: results of six months' follow-up. J Geriatr Cardiol 2023; 20(7): 495−508. DOI: 10.26599/1671-5411.2023.07.002.
Citation:
Please cite this article as: LI M, WEI N, SHI HY, JING XJ, KAN XH, GAO HQ, XIAO YL. Prevalence and clinical implications of polypharmacy and potentially inappropriate medication in elderly patients with heart failure: results of six months' follow-up. J Geriatr Cardiol 2023; 20(7): 495−508. DOI: 10.26599/1671-5411.2023.07.002.
Prevalence and clinical implications of polypharmacy and potentially inappropriate medication in elderly patients with heart failure: results of six months' follow-up
OBJECTIVES To investigate the prevalence of polypharmacy and potentially inappropriate medication (PIM) in elderly patients with heart failure (HF) and their impact on readmission and mortality.
METHODS We conducted a study of 274 participants aged 60 years or older with HF. The prevalence of polypharmacy (defined as the use of five or more medications) was calculated, and the 2019 American Geriatrics Society Beers criteria were applied to access PIMs. Medications and PIMs were characterized at admission and discharge, and changes in prescriptions during hospitalization were compared. The impact of polypharmacy and PIM on readmission and mortality were investigated.
RESULTS The median age of this study population was 68 years old. The median number of prescribed drugs was 7 at admission and 10 at discharge. At discharge, 99.27% of all patients were taking five or more drugs. The incidence of composite endpoint and cardiovascular readmission increased with the number of polypharmacy within 6 months. The use of guideline-directed medical therapy reduced the incidence of composite endpoint events and cardiovascular readmission, while the use of non-cardiovascular medications increased the composite endpoint events. The frequency of PIMs was 93.79% at discharge. The incidence of composite endpoint events increased with the number of PIMs. “PIMs in older adults with caution” increased cardiovascular readmission and “PIMs based on kidney function” increased cardiovascular mortality. Several comorbidities were associated with cardiovascular mortality or non-cardiovascular readmission.
CONCLUSIONS Polypharmacy and PIM were highly prevalent in elderly patients with HF, and their use was associated with an increased risk of composite endpoint events, readmission and mortality. Non-cardiovascular medications, “PIMs in older adults with caution”, “PIMs based on kidney function” and several comorbidities were important factors associated with hospital readmission and mortality. Our findings highlight the importance of medication optimization in the management of HF in elderly patients.
Heart failure (HF) is a complex clinical syndrome associated with high mortality, poor quality of life, and significant burden on the healthcare systems.[1-5] Hospitalization due to HF is common in the elderly population.[6] Aging is a major risk factor for HF, and it is projected that by 2050, the proportion of the world's population over 60 years old will reach 22%, which is twice the current proportion.[7] In China, the proportion is predicted to reach 34.1% of the total population.[8] Despite the increased use of guideline-directed medical therapy (GDMT) for HF,[9] it remains a leading cause of readmission and mortality globally in older adults globally.[4]
Polypharmacy, the use of multiple medications, is common in elderly patients with multiple chronic conditions. Approximately 30% of older adults take at least 5 or more medications.[10, 11] Polypharmacy is associated with adverse effects including functional decline,mortality, falls, adverse drug reactions, hospitalizations and increased length of hospital stay.[12-14] The risk of adverse effects is increased with the number of drugs taken.[15] However few studies have investigated the prevalence of polypharmacy and its influence on hospitalized elderly HF patients.[16]
Polypharmacy in elderly individuals with multiple health conditions is susceptible to potentially inappropriate medication (PIM).[17] PIM refers to medications that pose greater risks than benefits, especially when a safer or more effective alternative treatment is available for the same medical condition. Reducing or avoiding the use of PIM is a key intervention in managing elderly patients, particularly those with HF.
Several assessment tools have been developed to identify and prevent PIM. Among these, the American Geriatrics Society (AGS) Beers Criteria (last updated in 2019) is widely used as a guideline to evaluate the appropriateness of medications in older adults. It contains a list of PIMs that should be avoided due to their high risk and limited benefit, unless there are no safer or more effective alternatives available.[18] Previous studies have shown that the prevalence of PIM use in old adults is associated with adverse drug reactions, hospitalization, and increased healthcare costs.[19-24] However, limited research has been conducted on PIM use in elderly patients with HF, emphasizing the need for more comprehensive studies to evaluate the potential adverse outcomes associated with PIM use and to optimize prescribed medications.
In this context, the primary aim was to determine the prevalence of polypharmacy and PIM in elderly patients hospitalized for HF. The secondary objective was to examine the impact of polypharmacy and PIM on readmission and mortality in this population, with ultimate goal of providing specific recommendations for deprescribing and management of HF in the elderly.
METHODS
Study Population
This was a retrospective, single-center observational study conducted at the Geriatric Department of Qilu Hospital, a national regional geriatric medical center and tertiary hospital, affiliated with Shandong University, Jinan, China. As the study was retrospective, there were no prespecified criteria for setting assignments. The primary study included 274 seniors aged 60 years or older, who were hospitalized between September 2020 and July 2021 for HF with left ventricular ejection fraction (LVEF) less than 50%. In addition to baseline information related to health behaviors and medical history, follow-up data related to all-cause readmission and mortality, cardiovascular readmission, cardiovascular mortality and non-cardiovascular readmission were collected through routine telephone calls with participants and/or their relatives in the next 6 months after discharge. Participants’ medication data were examined at both admission and discharge.
Medical records of each adjudicated HF were reviewed and abstracted to collect information on medical conditions, admission and discharge vital signs, laboratory values, echocardiogram parameters (including LVEF), discharge disposition, length of stay and hospital-based events (including cardiac arrest and mechanical ventilation).
HF with reduced ejection fraction (HFrEF) is characterized by LVEF of 40% or less, indicating abnormal systolic function.[9] Participants with mildly reduced ejection fraction (LVEF: 41%-49%) were also included in the analysis and grouped with those with HFrEF given the shared pathophysiologic features.[25] Echocardiograms were performed during the hospitalization to determine the LVEF and/or qualitative description of systolic function.
Medications prescribed at admission and discharge were collected, including both prescribed and over-the-counter medications, as they contributed to medication and complexity.
The medications included in this study were for HF, non-HF related cardiovascular and non-cardiovascular management. Treatment for HF included GDMT, diuretics, anti-angina, calcium channel blockers (CCB), ivabradine and digoxin. GDMT for HF refers to renin-angiotensin system inhibition including angiotensin-converting enzyme inhibitors (ACEI) or angiotensin (II) receptor blockers (ARB) or angiotensin receptor-neprilysin inhibitors (ARNi), beta blockers (BB), sodium-glucose cotransporter 2 inhibitors (SGLT2i), and mineralocorticoid receptor antagonist (MRA).[9]
The study protocol was approved by medical ethics committee of Qilu Hospital of Shandong University (approval number: 2020(086)), and all subjects provided written informed consent at enrollment. The investigation adhered to the principles outlined in the Declaration of Helsinki.
Polypharmacy
Polypharmacy refers to the use of multiple medications, but there is no standardized definition yet. The most commonly used descriptive definition of polypharmacy is when an individual is prescribed 5 or more medications at the same time and on a daily basis.[26, 27] For this study, we defined the use of 10 or more medications as hyper-polypharmacy. Prescriptions were classified into 3 groups based on the number of medications prescribed: 1 to 4 medications (no polypharmacy), 5 to 9 medications, and 10 or more medications (hyperpolypharmacy).[11]
PIMs
PIMs (potentially inappropriate medication) were categorized into five groups based on the 2019 AGS Beers criteria: PIMs in older adults (PIM1); drug-disease or drug-syndrome PIMs (PIM2); PIMs in older adults with caution (PIM3); drug-drug interactions (PIM4); PIMs based on renal function (PIM5).[18] The PIM use was evaluated for the entire hospitalization period and at discharge for all the participants. In this study, patients were grouped into four categories based on the number of PIM: 0 PIM (no PIMs), 1 to 2 PIMs, 3 to 4 PIMs and PIMs ≥ 5.
Study Outcomes
The primary outcome measure in this study was a composite of all-cause readmission and death within a 6-month follow-up period. The secondary outcome measure was cardiovascular readmission, cardiovascular death or non-cardiovascular readmission within the same follow-up period.
Statistical Analysis
To summarize participant characteristics, hospital characteristics, and medication patterns, medians and interquartile ranges (IQRs) were calculated for continuous variables and percentages were calculated for categorical variables. For non-normal distribution variables, the Mann-Whitney U test was used for further analyses. The chi-square test and Fisher exact test were applied to compare nominal categorical variables.
Multiple logistic regression analysis after correlation analysis was conducted to identify independent factors associated with readmission and mortality. The following variables were included in the multiple logistic regression model: body index, coronary vascular disease, hypertension, diabetes, ventricular arrhythmia (VT), cerebrovascular disease, valvulopathy, atrial fibrillation/flutter (AF), chronic obstructive pulmonary disease (COPD)/pulmonary infection, the number of diagnosed diseases, the number of prescribed medications and PIMs. A P of less than 0.05 was considered statistically significant. All statistical analyses were performed using SPSS 25.0.
RESULTS
Participant Characteristics
We enrolled a total of 274 participants with a median age of 68 years old (IQR = 63−75); of whom 63.9% were male. The median length of hospital stay was 12 days (IQR = 9−16) as shown in Table 1. The median number of comorbidities was 4 (IQR = 3−6). Specifically, 74.1% (n = 203) had 1 to 5 comorbidities, 24.8% (n = 68) had 6 to 10, and only 1.1% (n = 3) had 11 or more comorbidities, as presented in Table1. The top 6 most prevalent comorbidities were coronary artery disease (79.93%), hypertension (53.3%), diabetes (38.7%), VT (31.75%), COPD/pulmonary infection (30.7%), and AF (24.5%), as reported in Table 1.
Table
1.
Characteristics of 274 elderly participants with heart failure.
Characteristics
Overall
Male
175 (63.9%)
Age, yrs
60-74
199 (72.6%)
75-84
58 (21.2%)
≥ 85
17 (6.2%)
Age, yrs
68 (63-75)
Length of hospital stay, day
1-5
8 (2.9%)
6-10
88 (32.1%)
≥ 11
178 (64.0%)
Length of hospital stay, day
12 (9-16)
No. polypharmacy at admission
1-4
48 (17.5%)
5-9
170 (62.0%)
≥ 10
56 (20.4%)
No. polypharmacy at admission
7 (5-9)
No. polypharmacy at discharge
1-4
2 (0.7%)
5-9
130 (47.5%)
≥ 10
142 (51.8%)
No. polypharmacy at discharge
10 (8-12)
No. comorbidities
1-5
203 (74.1%)
6-10
68 (24.8%)
≥ 11
3 (1.1%)
No. comorbidities
4 (3-6)
Comorbidities
Coronary artery disease
219 (79.9%)
Hypertension
146 (53.3%)
Diabetes
106 (38.7%)
Ventricular arrhythmia
87 (31.8%)
COPD/pulmonary infection
84 (30.7%)
AF
67 (24.5%)
Cerebrovascular disease
61 (22.3%)
DCM of unknown origin
52 (19.0%)
Valvulopathy
43 (15.7%)
Gallbladder system disease
31 (11.3%)
Abnormal liver and/or kidney function
28 (10.2%)
Cancer
25 (9.1%)
Gastric or duodenal ulcers
23 (8.4%)
Benign prostatic hyperplasia
15 (5.5%)
Peripheral vascular disease
13 (4.7%)
Depression
4 (1.5%)
Eye conditions
5 (1.8%)
Gout
3 (1.1%)
Data are presented as n (%) or median (IQR). AF: atrial fibrillation/flutter; COPD: chronic obstructive pulmonary disease; DCM: dilated cardiomyopathy; IQR: interquartile ranges.
The total number of medications for all participants was 1995 at admission and 2763 at discharge (Table 2). The median number of medications per patient was 7 (IQR = 5-9) at admission and 10 (IQR = 8-12) at discharge. Overall, at admission, 17.5% of all patients had less than 5 medications, 62.04% had 5 to 9 medications, and 20.4% had 10 or more medications (hyper-polypharmacy). At discharge, the proportions of all patients with less than 5 medications, 5 to 9 medications, hyper-polypharmacy were 0.7%, 47.5%, and 51.8%, respectively (Table 1). The total number of HF-related medications, non-HF cardiovascular and non-cardiovascular medications were 802 (40.2%), 766 (38.4%), 432 (21.7%) at admission and 1164 (42.1%), 915 (33.1%), 690 (25.0%) at discharge, respectively (Table 2).
Table
2.
Polypharmacy at admission and discharge.
Variable
Admission (n)
Discharge (n)
Change (%)
Polypharmacy
1995
2763
38.5*
HF-related medications
802
1164
45.1*
GDMT
513
684
33.3*
BB
207
248
19.8
MRA
160
232
45.0
ACEI/ARB
94
81
−13.8
ARNi
47
117
148.9
SGLT2i
5
6
20.0
Other HF-related medications
289
480
66.1*
Anti-angina (Nitrates, Nicorandil)
115
114
0.9
Diuretics
85
245
188.2
CCB
38
29
−23.7
Ivabradine
32
52
62.5
Digoxin
19
40
110.5
Non-HF cardiovascular
766
915
19.5*
Platelet inhibitors
314
290
−7.6
Anticoagulants
42
69
64.3
Lipid modifying agents
206
252
22.3
Others (trimetazidine, coenzyme Q10, etc.)
172
240
39.5
Cardiovascular Chinese patent drugs
32
64
100.0
Non-cardiovascular
432
690
60.0*
PPI
83
104
25.3
Blood glucose lowering drugs
121
156
29.3
Electrolyte supplements
38
87
129.0
Hypnotics
27
23
−14.8
Non-cardiovascular Chinese patent drugs
20
50
150.0
Others **
143
270
88.8
*P-values less than 0.05; **Others included liver, bile therapy, other nervous system drugs, etc. ACEI: angiotensin-converting enzyme inhibitors; ARB: angiotensin (II) receptor blockers; ARNi: angiotensin receptor-neprilysin inhibitors; BB: beta blockers; CCB: calcium channel blockers; GDMT: guideline-directed medical therapy; HF: heart failture; MRA: mineralocorticoid receptor antagonist; PPI: proton pump inhibitors; SGLT2i: sodium-glucose cotransporter 2 inhibitor.
Lipid-modifying agents and beta blocking agents were the most commonly used medications at both admission and discharge. The number of prescriptions for amiodarone, furosemide, and ARNi increased the most from admission to discharge (Table 2). The use of guideline-directed medical therapy (GDMT) increased by 33.33% at discharge. Among all GDMT, the use of ARNi increased most noticeably at discharge (Table 2).
At discharge, we only compared the two polypharmacy groups: 5 to 9 and hyper-polypharmacy, as only one patient was prescribed with less than 5 medications. The proportion of male patients in hyper-polypharmacy was higher than that of 5 to 9 group (70.4% vs. 56.9%, P = 0.021). The mean age of all patients in hyper-polypharmacy group was older than that of the 5 to 9 group, but the difference was not statistically significant (68.6 vs. 70.4, P = 0.053). The mean number of comorbidities in the hyperpolypharmacy group was higher than that of the 5 to 9 group (4.6 vs. 3.9, P < 0.001). The proportions of the patients with combined coronary vascular disease, hypertension and diabetes in the hyper-polypharmacy group were higher than those in the 5 to 9 group (85.2% vs. 67.4%, P = 0.001; 64.8% vs. 40.2%, P < 0.001; 44.4% vs. 22.7%, P < 0.001, respectively) (Table 3).
Table
3.
Influence of baseline characteristics on polypharmacy and hyper-polypharmacy.
Variable
Polypharmacy 5-9, n = 130
Polypharmacy ≥ 10, n = 142
P-value
Male
74 (56.9%)
100 (70.4%)
0.021*
Age, yrs
68.6
70.2
0.053
BMI, kg/m2
23.8
24.6
0.119
No. diagnosed disease
3.9
4.6
< 0.001*
Coronary vascular disease
89 (67.4%)
121 (85.2%)
0.001*
Hypertension
53 (40.2%)
92 (64.8%)
< 0.001*
Diabetes
30 (22.7%)
63 (44.4%)
< 0.001*
PVC/VT
40 (30.3%)
49 (34.5%)
0.776
AF
39 (29.6%)
25 (17.6%)
0.011*
Myocardiopathy unknown origin
36 (27.3%)
15 (10.6%)
< 0.001*
Length of hospital stay, day
12.7
14.2
0.065
Composite endpoint
13.9%
21.8%
0.034*
Cardiovascular re-admission
12.3%
16.2%
0.039*
Cardiovascular death
3.1%
1.4%
0.714
AF: atrial fibrillation/flutter; PIM: potentially inappropriate medication; PVC: premature ventricular contraction; VT: ventricular tachycardia. The composite endpoint was all-cause death and readmission; * Factors with P-values less than 0.05.
During the 6-month follow-up after discharge, patients in the hyperpolypharmacy group had higher incidences of the composite endpoint and cardiovascular readmission compared to those in the 5 to 9 group (21.8% vs. 13.9%, P = 0.034; 16.2% vs. 12.3%, P = 0.039, respectively). The difference between 5 to 9 medications and hyperpolypharmacy group was not statistically significant in the incidence of cardiovascular death (1.4% vs. 3.1%, P = 0.714) (Table 3).
PIMs
According to the 2019 AGS Beers criteria, a total of 340 PIMs were identified at admission, and 693 PIMs were identified at discharge in all participants. The most frequently encountered PIMs category was “PIMs to be used with caution” (35.8%), followed by “PIMs in older adults” (32.3%), “drug-drug interactions” (28.4%), “PIMs based on kidney function” (3.0%) and “drug-disease and drug-syndrome PIMs” (0.4%) at discharge. Furosemide (n = 177), ACEI/ARB-ARNi-spironolactone (n = 171) and proton pump inhibitors (PPI) (n = 104) were the top 3 most frequently encountered PIMs at discharge. Furosemide belonged to “PIMs to be used with caution” category and accounted for 71.4% of this category at discharge. ACEI/ARB-ARNi-spironolactone belonged to the “drug-drug interactions” category and accounted for 86.8% of this category at discharge. PPI belonged to “PIMs in older adults” category and accounted for 46.4% of this category at discharge. During hospitalization, the greatest increase in all categories was observed for “PIMs to be used with caution” (from 86 to 248), followed by “drug-drug interactions” (from 89 to 197) (Table 4).
Table
4.
Prevalence of PIMs based on the 2019 AGS Beers criteria.
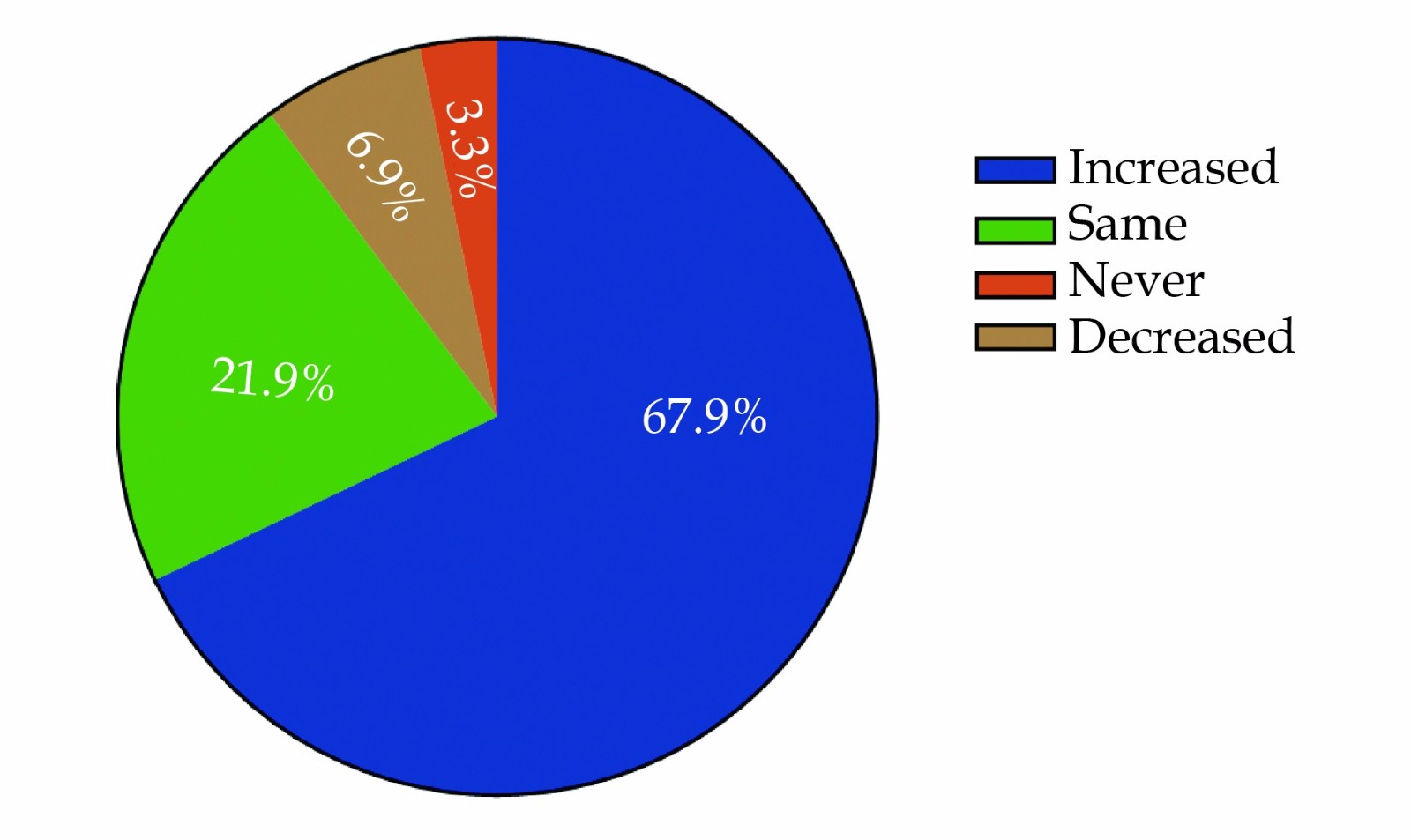
Compared to admission, 67.9% of all patients experienced an increase in the number of PIMs, while only 6.9% of all patients had a decrease in the number of PIMs. Approximately 21.9% of all patients remained on the same number of PIMs at discharge, and 3.3% of all patients were never prescribed PIMs at either admission or discharge (Figure 1).
Figure
1.
Prescription of potentially inappropriate medication.
We conducted a comparison of four PIM groups: 0 PIM (no PIMs), 1 to 2 PIMs, 3 to 4 PIMs, and PIMs ≥ 5. Participants in the PIMs ≥ 5 group had a higher mean age of 75.4 years old compared to the other groups (P = 0.002). The average length of hospital stay in the PIMs ≥ 5 group was 17.3 days, which was longer than the other groups (P = 0.022). Additionally, the average number of diagnosed diseases in the PIMs ≥ 5 group was 6.40, which was higher than the other groups (P < 0.001). Within 6 months follow-up after discharge, the incidence of the composite endpoint was higher in the PIMs ≥ 5 group compared to the other groups (P = 0.03). Although the incidence of cardiovascular readmission was also higher in the PIMs ≥ 5 group, there was no statistical significance (P = 0.072). Furthermore, the proportion of PIMs ≥ 5 group combined with hypertension was higher than the other groups (P = 0.023) (Table 5).
Table
5.
Influence of baseline characteristics on PIM#.
Variable
PIMs 0, n = 17
PIMs 1-2, n = 126
PIMs 3-4, n = 111
PIMS ≥ 5, n = 20
P-value
Male
70.6%
67.5%
55.9%
80.0%
0.095
Age, yrs
68.4
68.3
70.4
75.4
0.002*
BMI, kg/m2
22.8
24.6
24.3
25.4
0.318
Length of hospital stay, day
14.9
12.9
13.3
17.3
0.022*
No. average diagnosed disease
3.6
4.3
4.4
6.4
< 0.001*
Mean medications
6.5
9.2
11.1
14.4
< 0.001*
Coronary vascular disease
88.2%
74.6%
74.8%
95.0%
0.129
Hypertension
47.1%
48.4%
54.1%
85.0%
0.023*
Diabetes
23.5%
34.1%
30.6%
55.0%
0.146
PVC/VT
17.7%
14.3%
23.4%
20.0%
0.146
AF
23.5%
21.4%
22.5%
40.0%
0.381
Myocardiopathy unknown origin
5.9%
21.4%
20.7%
0
0.041*
Composite endpoint
5.9%
15.9%
25.2%
30.0%
0.030*
Cardiovascular readmission
0
12.7%
19.8%
20.0%
0.072
#All patients were categorized into 4 groups according to the number of PIM: 0 PIM (no PIMs), 1 to 2 PIMs, 3 to 4 PIMs and PIMs ≥ 5. *Factors with P-values less than 0.05. AF: atrial fibrillation/flutter; BMI: body mass index; PIM: potentially inappropriate medication; PVC: premature ventricular contraction; VT: ventricular tachycardia. The composite endpoint was all-cause death and readmission.
Influence of Polypharmacy and PIM on Readmission and Mortality of HF in Elderly Patients
In the correlation analysis and multiple logistic regression analysis, several variables were found to be associated with the composite endpoint, including polypharmacy (P = 0.007, OR = 1.135), PIMs (P = 0.010, OR = 1.155), AF (P = 0.043, OR = 1.971) and myocardiopathy of unknown origin (P = 0.028, OR = 1.302), use of GDMT (P = 0.023, OR = 0.707) and use of non-cardiovascular medications (P = 0.010, OR = 1.155) (see Tables 6 for details).
Table
6.
Multiple logistic regression analysis of factors associated with composite endpoint.
Variables
b
S.E.
Wals
df
Sig
OR
Polypharmacy
0.127
0.047
7.168
1
0.007*
1.135
GDMT
0.535
0.235
5.187
1
0.023*
0.707
HF medications
0.211
0.109
3.773
1
0.052
1.235
Non cardiovascular
0.144
0.056
6.564
1
0.010*
1.155
Overall PIMs
0.265
0.090
8.769
1
0.003*
1.304
PIM3
0.440
0.189
5.392
1
0.020*
1.552
PIM4
0.537
0.276
3.780
1
0.052
1.711
PIM5
0.901
0.399
5.108
1
0.024*
2.463
No. diagnosed disease
0.113
0.067
2.818
1
0.093
1.120
Diabetes
0.378
0.235
2.581
1
0.108
1.459
Myocardiopathy unknown origin
−1.197
0.545
4.818
1
0.028*
1.302
AF
0.679
0.335
4.114
1
0.043*
1.971
AF: atrial fibrillation/flutter; GDMT: guideline-directed medical therapy; PIM3: PIMs in older adults with caution; PIM4: drug-drug interactions; PIM5: PIMs based on renal function. *Factors with P-values less than 0.05.
The following variables were found to be associated with cardiovascular readmission: use of GDMT (P = 0.044, OR = 0.737), “PIMs based on kidney function” (P = 0.018, OR = 1.697) and AF (P = 0.033, OR = 2.220) (Table 7). Cardiovascular death was associated with “PIMs based on kidney function” (P = 0.014, OR = 4.188) and cerebrovascular diseases (P = 0.036, OR = 5.139) (Table 8). Non-cardiovascular readmission was associated with the comorbidity of gastric or duodenal ulcers (P = 0.015, OR = 6.125) (Table 9).
Table
7.
Multiple logistic regression analysis of factors associated with cardiovascular readmission.
Variables
b
S.E.
Wals
df
Sig
OR
GDMT
0.552
0.273
4.074
1
0.044*
0.737
HF medications
0.243
0.125
3.780
1
0.052
1.274
Overall PIMs
0.179
0.099
3.250
1
0.071
1.196
PIM3
0.529
0.224
5.556
1
0.018*
1.697
No. diagnosed disease
0.096
0.076
1.589
1
0.207
1.101
BMI
−0.055
0.044
1.564
1
0.211
0.947
Coronary vascular disease
0.085
0.450
0.035
1
0.851
1.088
Hypertension
0.036
0.355
0.010
1
0.920
1.036
Diabetes
0.479
0.252
3.604
1
0.058
1.615
Myocardiopathy unknown origin
−1.083
0.623
3.020
1
0.082
0.339
Valvulopathy
−0.454
0.558
0.663
1
0.416
0.635
AF
0.797
0.374
4.546
1
0.033*
2.220
PVC/VT
−0.075
0.411
0.034
1
0.854
0.927
Cerebrovascular disease
0.184
0.415
0.197
1
0.657
1.202
Gastric or duodenal ulcers
−0.044
0.646
0.005
1
0.946
0.957
COPD/pulmonary infection
0.126
0.365
0.120
1
0.729
1.135
Cancer
−1.333
1.025
1.693
1
0.193
0.264
*Factors with P-values less than 0.05. AF: atrial fibrillation/flutter; BMI: body mass index; COPD: chronic obstructive pulmonary disease; GDMT: guideline-directed medical therapy; HF: heart failure; PIM3: PIMs in older adults with caution; PVC: premature ventricular contraction; VT: ventricular tachycardia.
Table
8.
Multiple logistic regression analysis of factors associated with cardiovascular death.
Variables
b
S.E.
Wals
df
Sig
OR
PIM5
1.415
0.574
6.083
1
0.014*
4.118
BMI
−0.155
0.092
2.849
1
0.091
0.856
Hypertension
0.160
0.774
0.043
1
0.836
1.174
Diabetes
−0.255
0.773
0.109
1
0.742
0.775
Valvulopathy
0.820
0.854
0.921
1
0.337
2.270
AF
1.505
0.778
3.745
1
0.053
4.503
PVC/VT
0.806
0.777
1.077
1
0.299
2.239
Cerebrovascular disease
1.637
0.779
4.420
1
0.036*
5.139
COPD/pulmonary infection
−0.063
0.821
0.006
1
0.939
0.939
*Factors with P-values less than 0.05. BMI: body mass index; PIM5: PIMs based on renal function; PVC: premature ventricular contraction; VT: ventricular tachycardia.
Our study showed that polypharmacy and PIM were highly prevalent in elderly patients with HF, and their use was associated with an increased risk of composite endpoint events, readmission and mortality. Several studies have reported the outcomes of polypharmacy and PIM for elderly inpatients,[15,28-31] but not for elderly population with HF.
It has been reported that polypharmacy is highly prevalent among hospitalized elderly patients, with up to 70% routinely taking 5 or more medications in developed countries.[15, 32, 33] In a study by Unlu, et al.[16] focusing on elderly patients with HF, the vast majority of participants (84% at admission and 95% at discharge) took ≥ 5 medications, which is similar to our study (82.5% at admission and 99.3% at discharge). This means that almost every elderly patient with HF is exposed to polypharmacy at discharge. Notably, the proportion of polypharmacy in elderly patients with HF is significantly higher than that in other hospitalized elderly. In one study in China, 37.9% of elderly inpatients were regularly prescribed 10 or more medications.[34] In our study, which focused on the elderly patients with HF, 51.8% of all participants were prescribed 10 or more (hyper-polypharmacy) medications, which is higher than the proportion observed in the elderly inpatients, and similar to the findings of Ozan Unluet al. (55%).[16] Thus, polypharmacy, including hyper-polypharmacy, is more common and more serious in the elderly patients with HF. This may be attributed to the unique characteristics of HF itself and the elderly population. Our study showed that patients with hyper-polypharmacy were older, predominantly male, and had more comorbidities, although these differences were not statistically significant. Therefore, there is an urgent need to further investigate polypharmacy in elderly patients with HF.
Polypharmacy has been found to be significantly associated with negative health outcomes, such as adverse drug events, cognitive decline, hospitalization, and even death, especially in elderly inpatients.[15,28-31,35] Previous studies have also shown that polypharmacy significantly increased the risk of hospital readmission within 30 days after discharge in hospitalized elderly patients.[29,31,35,36] However there is limited real-world data on polypharmacy and its associated hospital readmission and mortality in the setting of elderly patients with HF. In our study, which followed patients for 6 months, polypharmacy was associated with a higher risk of the composite endpoint (all-cause readmission and death) and patients with hyper-polypharmacy had even higher odds of the composite endpoint and cardiovascular readmission. Therefore, it is important to avoid unnecessary polypharmacy to decrease negative outcomes. Our study also found that the incidence of adverse outcomes increased with the number of comorbidities, and patients with hyper-polypharmacy had more combined diseases, such as coronary vascular diseases, hypertension, diabetes or AF. These findings suggest the need for increased attention to HF patients with these comorbidities, as well as early involvement of multidisciplinary consultation clinical pharmacists in medication management to optimize prescribed medications.
A prior study has found that the incidence of PIM rose with the number of medications prescribed in inpatients aged 65 years or older.[37] However for the elderly patients with HF, the relationship between PIM and the number of medications was uncertain. In our study, PIM prevalence soared 73.4% in patients with hyper-polypharmacy, compared with that of the population of 5 to 9 drugs at discharge. 93.8% of participants with polypharmacy were in the state of PIMs at discharge, which implied that PIM was closely related with polypharmacy in the elderly with HF. More evidence-based medical research is urgent to reveal the relationship between polypharmacy and PIM in different diseases, especially for the elderly patients.
Jano, et al.[38] have reported that PIMs are significantly associated with negative clinical outcomes in older adults, including higher rates of mortality and hospitalizations, and are a preventable cause of negative clinical consequences in the elderly patients.[39] However, little research has been conducted on PIM and its associated adverse outcome in the elderly patients with HF. Our study reveals that PIM are a major risk factor of the composite endpoint (all-cause readmission and mortality) in this population. In addition, “PIMs to be used with caution” increased the risk of cardiovascular readmission, while “PIMs based on kidney function” played an important role in cardiovascular mortality. Therefore, medications belonging to those PIMs should be used with caution, especially in elderly patients with HF. This provides more targeted recommendations for optimizing prescribed medications.
To observe the influence of the number of PIMs on outcomes, we compared the composite endpoint, cardiovascular readmission and cardiovascular death within 6 months among different PIMs groups. We found that the number of composite endpoint events increased with the number of PIMs. In the higher PIM group, the average age of patients was 75.4 years old, which is higher than that of the other lower PIMs group. Therefore, patients with HF over 75 years old are more likely to have higher PIMs and may need to be further monitored to reduce the adverse effects of PIM. Additionally, in this group, the incidence of combined diseases was higher, including hypertension and myocardiopathy of unknown origin. Patients with HF who have multimorbidity, especially those with hypertension and myocardiopathy of unknown origin, are at high risk of having higher PIMs. Therefore, more attention should be paid to this subgroup of patients to reduce the negative outcomes of PIM. And also the patients with higher PIMs had longer length of hospital stay and worse outcomes. More attention should be paid to this population and their optimization of prescribed during the follow-up. All these data fill the gap in our understanding of the influence of PIM on the elderly patients with HF and provide more targeted approaches to reduce unnecessary PIM.
The changes in PIMs after discharge showed that the use of diuretics, particularly furosemide, increased significantly. Diuretics were often employed as a part of decongestion strategies to reduce the length of hospital stay in older adults hospitalized for with HF. However, their impact on HF mortality remains uncertain. In our study, diuretics were the most commonly prescribed medication in the “PIMs to be used with caution” category, accounting for 98.8% of the prescription. Although diuretics increased cardiovascular readmission, they didn’t increase composite endpoint events. Therefore, at present, diuretics should always be used in conjunction with GDMT in elderly patients with HF. However, in our study, we did not analyze the dose and type of diuretics or their impact on outcomes, hence further research is required.
The second most commonly used PIM category was ACEI/ARB-ARNi-Spironolactone, all of which were all GDMT for HF. The efficacy of GDMT has been established for the entire HF population, but no specific guidelines are available for the elderly HF patients. Therefore, more extensive research is needed to investigate the effects of GDMT in this population. In our study, GDMT was found to decrease the composite endpoint in elderly patients with HF. Thus, it is important to acknowledge that PIM may not always be inappropriate in certain diseases, and the use of GDMT should not be overly restricted in the elderly patients with HF. The 2019 AGS Beers Criteria, designed for the older adults in general, do not provide detailed guidance for specific conditions. Therefore, more attention should be paid to the association between PIMs and the specific diseases, and further clinical trials are necessary to refine criteria for different conditions.
PPIs are also commonly encountered in PIMs, but we found that non-cardiovascular medications, including PPIs, increased composite endpoint events. It is crucial to exercise caution in the use of non-cardiovascular medications, especially PPIs, and to prescribe them strictly based on their indications and contraindications. Thus, in the management of HF in the elderly patients, emphasis should not only be placed on the use of GDMT, but also on deprescribing of unnecessary non-cardiovascular medications. The strategies of a risk-benefit assessment and deprescribing should be incorporated into routine medication management.
One of the main strengths of this study was its real-world approach, which examined the impact of polypharmacy and PIM in the elderly patients with HF. Although our study was limited by its small sample size and single-center design in Shandong, which may have introduced some bias in the results, the advantage of monocentric design is the consistency it provides in therapy prescription criteria.
In conclusion, our study highlights the high prevalence of polypharmacy and PIM in elderly patients with HF. Within 6 months of follow-up, we found that the incidence of composite endpoint events (all-cause readmission and mortality) increased with the number of PIMs and medications prescribed. ACEI/ARB-ARNi-Spironolactone were commonly prescribed as PIMs and GDMT, and were found to reduce composite endpoint events in this population. Thus, the limiting the use of GDMT in elderly patients with HF should be avoided. Notably, the use of non-cardiovascular medications, “PIMs in older adults with caution” category, “PIMs based on kidney function” category, and comorbidities such as AF, cerebrovascular diseases, and gastric or duodenal ulcers were all associated with hospital readmission and mortality. Our study provided valuable insights into optimizing medication prescription in the elderly with HF.
Acknowledgments
The authors express their gratitude to all the hospital staff who assisted with data retrieval from the electronic medical record database and routine telephone follow-up. Additionally, the authors would like to extend their appreciation to Wenhui Liu for providing statistical guidance at the School of Public Health, Shandong University. The authors declare that they have no conflicts of interests to disclose.
Savarese G, Becher PM, Lund LH, et al. Global burden of heart failure: A comprehensive and updated review of epidemiology. Cardiovasc Res 2023; 118: 3272−3287. doi: 10.1093/cvr/cvac013
[2]
Dharmarajan K, Rich MW. Epidemiology, pathophysiology, and prognosis of heart failure in older adults. Heart Fail Clin 2017; 13: 417−426. doi: 10.1016/j.hfc.2017.02.001
[3]
Costantino S, Paneni F, Cosentino F. Ageing, metabolism and cardiovascular disease. J Physiol 2016; 594: 2061−2073. doi: 10.1113/JP270538
[4]
Diez-Villanueva P, Jimenez-Mendez C, Alfonso F. Heart failure in the elderly. J Geriatr Cardiol 2021; 18: 219−232.
[5]
Díez-Villanueva P, Jiménez-Méndez C, Alfonso F. Heart failure in the elderly. J Geriatr Cardiol 2021; 18: 219−232.
[6]
El Hadidi S, Rosano G, Tamargo J, et al. Potentially inappropriate prescriptions in heart failure with reduced ejection fraction: ESC position statement on heart failure with reduced ejection fraction-specific inappropriate prescribing. Eur Heart J Cardiovasc Pharmacother 2022; 8: 187−210. doi: 10.1093/ehjcvp/pvaa108
[7]
Kanasi E, Ayilavarapu S, Jones J. The aging population: demographics and the biology of aging. Periodontol 2000 2016; 72: 13−18. doi: 10.1111/prd.12126
[8]
Fu X, Sun N, Xu F, et al. Influencing factors of inequity in health services utilization among the elderly in China. Int J Equity Health 2018; 17: 144. doi: 10.1186/s12939-018-0861-6
[9]
Writing Committee Members. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure. J Card Fail 2022; 28: e1−e167. doi: 10.1016/j.cardfail.2022.02.010
[10]
Kim J, Parish AL. Polypharmacy and medication management in older adults. Nurs Clin North Am 2017; 52: 457−468. doi: 10.1016/j.cnur.2017.04.007
[11]
Hilmer SN, Gnjidic D. The effects of polypharmacy in older adults. Clin Pharmacol Ther 2009; 85: 86−8. doi: 10.1038/clpt.2008.224
[12]
Mekonnen AB, Redley B, De Courten B, et al. Potentially inappropriate prescribing and its associations with health-related and system-related outcomes in hospitalised older adults: A systematic review and meta-analysis. Br J Clin Pharmacol 2021; 87: 4150−4172. doi: 10.1111/bcp.14870
[13]
Sganga F, Vetrano DL, Volpato S, et al. Physical performance measures and polypharmacy among hospitalized older adults: results from the CRIME study. J Nutr Health Aging 2014; 18: 616−621. doi: 10.1007/s12603-014-0029-z
[14]
Fabbietti P, Ruggiero C, Sganga F, et al. Effects of hyperpolypharmacy and potentially inappropriate medications (PIMs) on functional decline in older patients discharged from acute care hospitals. Arch Gerontol Geriatr 2018; 77: 158−162. doi: 10.1016/j.archger.2018.05.007
[15]
Maher RL, Hanlon J, Hajjar ER. Clinical consequences of polypharmacy in elderly. Expert Opin Drug Saf 2014; 13: 57−65.
[16]
Unlu O, Levitan EB, Reshetnyak E, et al. Polypharmacy in older adults hospitalized for heart failure. Circ Heart Fail 2020; 13: e006977. doi: 10.1161/CIRCHEARTFAILURE.120.006977
[17]
Pages A, Rouch L, Costa N, et al. Potentially inappropriate medication prescribing detected by computer algorithm among older patients: results from the MAPT study. Pharmacy (Basel) 2021; 9: 189.
[18]
By the American Geriatrics Society Beers Criteria Update Expert P. American Geriatrics Society 2019 Updated AGS Beers Criteria(R) for Potentially Inappropriate Medication Use in Older Adults. J Am Geriatr Soc 2019; 67: 674−694. doi: 10.1111/jgs.15767
[19]
Muhlack DC, Hoppe LK, Weberpals J, et al. The association of potentially inappropriate medication at older age with cardiovascular events and overall mortality: a systematic review and meta-analysis of cohort studies. J Am Med Dir Assoc 2017; 18: 211−220. doi: 10.1016/j.jamda.2016.11.025
[20]
Lu WH, Wen YW, Chen LK, et al. Effect of polypharmacy, potentially inappropriate medications and anticholinergic burden on clinical outcomes: a retrospective cohort study. CMAJ 2015; 187: E130−E137. doi: 10.1503/cmaj.141219
[21]
Lin HY, Liao CC, Cheng SH, et al. Association of potentially inappropriate medication use with adverse outcomes in ambulatory elderly patients with chronic diseases: experience in a Taiwanese medical setting. Drugs Aging 2008; 25: 49−59. doi: 10.2165/00002512-200825010-00006
[22]
Skoldunger A, Fastbom J, Wimo A, et al. Impact of inappropriate drug use on hospitalizations, mortality, and costs in older persons and persons with dementia: findings from the SNAC study. Drugs Aging 2015; 32: 671−678. doi: 10.1007/s40266-015-0287-4
[23]
Harrison SL, Kouladjian O'donnell L, Milte R, et al. Costs of potentially inappropriate medication use in residential aged care facilities. BMC Geriatr 2018; 18: 9. doi: 10.1186/s12877-018-0704-8
[24]
Heider D, Matschinger H, Meid AD, et al. The impact of potentially inappropriate medication on the development of health care costs and its moderation by the number of prescribed substances. Results of a retrospective matched cohort study. PLoS One 2018; 13: e0198004.
[25]
Butler J, Anker SD, Packer M. Redefining heart failure with a reduced ejection fraction. JAMA 2019; 322: 1761−1762. doi: 10.1001/jama.2019.15600
[26]
Masnoon N, Shakib S, Kalisch-Ellett L, et al. What is polypharmacy? A systematic review of definitions. BMC Geriatr 2017; 17: 230. doi: 10.1186/s12877-017-0621-2
[27]
Viktil KK, Blix HS, Moger TA, et al. Polypharmacy as commonly defined is an indicator of limited value in the assessment of drug-related problems. Br J Clin Pharmacol 2007; 63: 187−195. doi: 10.1111/j.1365-2125.2006.02744.x
[28]
Wastesson JW, Morin L, Tan ECK, et al. An update on the clinical consequences of polypharmacy in older adults: a narrative review. Expert Opin Drug Saf 2018; 17: 1185−1196. doi: 10.1080/14740338.2018.1546841
[29]
Basnet S, Zhang M, Lesser M, et al. Thirty-day hospital readmission rate amongst older adults correlates with an increased number of medications, but not with Beers medications. Geriatr Gerontol Int 2018; 18: 1513−1518. doi: 10.1111/ggi.13518
[30]
Wu Y, Zhu W, He X, et al. Influence of polypharmacy on patients with heart failure with preserved ejection fraction: a retrospective analysis on adverse outcomes in the TOPCAT trial. Br J Gen Pract 2021; 71: e62−e70. doi: 10.3399/bjgp21X714245
[31]
Pereira F, Verloo H, Zhivko T, et al. Risk of 30-day hospital readmission associated with medical conditions and drug regimens of polymedicated, older inpatients discharged home: a registry-based cohort study. BMJ Open 2021; 11: e052755. doi: 10.1136/bmjopen-2021-052755
[32]
Reeve E, Gnjidic D, Long J, et al. A systematic review of the emerging de fi nition of 'deprescribing' with network analysis: implications for future research and clinical practice. Br J Clin Pharmacol 2015; 80: 1254−1268. doi: 10.1111/bcp.12732
[33]
Payne RA, Avery AJ, Duerden M, et al. Prevalence of polypharmacy in a Scottish primary care population. Eur J Clin Pharmacol 2014; 70: 575−581. doi: 10.1007/s00228-013-1639-9
[34]
Zhang X, Zhou S, Pan K, et al. Potentially inappropriate medications in hospitalized older patients: a cross-sectional study using the Beers 2015 criteria versus the 2012 criteria. Clin Interv Aging 2017; 12: 1697−1703. doi: 10.2147/CIA.S146009
[35]
Glans M, Kragh Ekstam A, Jakobsson U, et al. Medication-related hospital readmissions within 30 days of discharge-A retrospective study of risk factors in older adults. PLoS One 2021; 16: e0253024. doi: 10.1371/journal.pone.0253024
[36]
Fabbietti P, Di Stefano G, Moresi R, et al. Impact of potentially inappropriate medications and polypharmacy on 3-month readmission among older patients discharged from acute care hospital: a prospective study. Aging Clin Exp Res 2018; 30: 977−984. doi: 10.1007/s40520-017-0856-y
[37]
Tao L, Qu X, Gao H, et al. Polypharmacy and potentially inappropriate medications among elderly patients in the geriatric department at a single-center in China: A retrospective cross-sectional study. Medicine (Baltimore) 2021; 100: e27494. doi: 10.1097/MD.0000000000027494
[38]
Jano E, Aparasu RR. Healthcare outcomes associated with beers' criteria: a systematic review. Ann Pharmacother 2007; 41: 438−447. doi: 10.1345/aph.1H473
[39]
Gutierrez-Valencia M, Martinez-Velilla N, Vilches-Moraga A. Polypharmacy in older people: time to take action. Eur Geriatr Med 2019; 10: 1−3.
Table
1.
Characteristics of 274 elderly participants with heart failure.
Characteristics
Overall
Male
175 (63.9%)
Age, yrs
60-74
199 (72.6%)
75-84
58 (21.2%)
≥ 85
17 (6.2%)
Age, yrs
68 (63-75)
Length of hospital stay, day
1-5
8 (2.9%)
6-10
88 (32.1%)
≥ 11
178 (64.0%)
Length of hospital stay, day
12 (9-16)
No. polypharmacy at admission
1-4
48 (17.5%)
5-9
170 (62.0%)
≥ 10
56 (20.4%)
No. polypharmacy at admission
7 (5-9)
No. polypharmacy at discharge
1-4
2 (0.7%)
5-9
130 (47.5%)
≥ 10
142 (51.8%)
No. polypharmacy at discharge
10 (8-12)
No. comorbidities
1-5
203 (74.1%)
6-10
68 (24.8%)
≥ 11
3 (1.1%)
No. comorbidities
4 (3-6)
Comorbidities
Coronary artery disease
219 (79.9%)
Hypertension
146 (53.3%)
Diabetes
106 (38.7%)
Ventricular arrhythmia
87 (31.8%)
COPD/pulmonary infection
84 (30.7%)
AF
67 (24.5%)
Cerebrovascular disease
61 (22.3%)
DCM of unknown origin
52 (19.0%)
Valvulopathy
43 (15.7%)
Gallbladder system disease
31 (11.3%)
Abnormal liver and/or kidney function
28 (10.2%)
Cancer
25 (9.1%)
Gastric or duodenal ulcers
23 (8.4%)
Benign prostatic hyperplasia
15 (5.5%)
Peripheral vascular disease
13 (4.7%)
Depression
4 (1.5%)
Eye conditions
5 (1.8%)
Gout
3 (1.1%)
Data are presented as n (%) or median (IQR). AF: atrial fibrillation/flutter; COPD: chronic obstructive pulmonary disease; DCM: dilated cardiomyopathy; IQR: interquartile ranges.
Table
3.
Influence of baseline characteristics on polypharmacy and hyper-polypharmacy.
Variable
Polypharmacy 5-9, n = 130
Polypharmacy ≥ 10, n = 142
P-value
Male
74 (56.9%)
100 (70.4%)
0.021*
Age, yrs
68.6
70.2
0.053
BMI, kg/m2
23.8
24.6
0.119
No. diagnosed disease
3.9
4.6
< 0.001*
Coronary vascular disease
89 (67.4%)
121 (85.2%)
0.001*
Hypertension
53 (40.2%)
92 (64.8%)
< 0.001*
Diabetes
30 (22.7%)
63 (44.4%)
< 0.001*
PVC/VT
40 (30.3%)
49 (34.5%)
0.776
AF
39 (29.6%)
25 (17.6%)
0.011*
Myocardiopathy unknown origin
36 (27.3%)
15 (10.6%)
< 0.001*
Length of hospital stay, day
12.7
14.2
0.065
Composite endpoint
13.9%
21.8%
0.034*
Cardiovascular re-admission
12.3%
16.2%
0.039*
Cardiovascular death
3.1%
1.4%
0.714
AF: atrial fibrillation/flutter; PIM: potentially inappropriate medication; PVC: premature ventricular contraction; VT: ventricular tachycardia. The composite endpoint was all-cause death and readmission; * Factors with P-values less than 0.05.
Table
5.
Influence of baseline characteristics on PIM#.
Variable
PIMs 0, n = 17
PIMs 1-2, n = 126
PIMs 3-4, n = 111
PIMS ≥ 5, n = 20
P-value
Male
70.6%
67.5%
55.9%
80.0%
0.095
Age, yrs
68.4
68.3
70.4
75.4
0.002*
BMI, kg/m2
22.8
24.6
24.3
25.4
0.318
Length of hospital stay, day
14.9
12.9
13.3
17.3
0.022*
No. average diagnosed disease
3.6
4.3
4.4
6.4
< 0.001*
Mean medications
6.5
9.2
11.1
14.4
< 0.001*
Coronary vascular disease
88.2%
74.6%
74.8%
95.0%
0.129
Hypertension
47.1%
48.4%
54.1%
85.0%
0.023*
Diabetes
23.5%
34.1%
30.6%
55.0%
0.146
PVC/VT
17.7%
14.3%
23.4%
20.0%
0.146
AF
23.5%
21.4%
22.5%
40.0%
0.381
Myocardiopathy unknown origin
5.9%
21.4%
20.7%
0
0.041*
Composite endpoint
5.9%
15.9%
25.2%
30.0%
0.030*
Cardiovascular readmission
0
12.7%
19.8%
20.0%
0.072
#All patients were categorized into 4 groups according to the number of PIM: 0 PIM (no PIMs), 1 to 2 PIMs, 3 to 4 PIMs and PIMs ≥ 5. *Factors with P-values less than 0.05. AF: atrial fibrillation/flutter; BMI: body mass index; PIM: potentially inappropriate medication; PVC: premature ventricular contraction; VT: ventricular tachycardia. The composite endpoint was all-cause death and readmission.
Table
6.
Multiple logistic regression analysis of factors associated with composite endpoint.
Variables
b
S.E.
Wals
df
Sig
OR
Polypharmacy
0.127
0.047
7.168
1
0.007*
1.135
GDMT
0.535
0.235
5.187
1
0.023*
0.707
HF medications
0.211
0.109
3.773
1
0.052
1.235
Non cardiovascular
0.144
0.056
6.564
1
0.010*
1.155
Overall PIMs
0.265
0.090
8.769
1
0.003*
1.304
PIM3
0.440
0.189
5.392
1
0.020*
1.552
PIM4
0.537
0.276
3.780
1
0.052
1.711
PIM5
0.901
0.399
5.108
1
0.024*
2.463
No. diagnosed disease
0.113
0.067
2.818
1
0.093
1.120
Diabetes
0.378
0.235
2.581
1
0.108
1.459
Myocardiopathy unknown origin
−1.197
0.545
4.818
1
0.028*
1.302
AF
0.679
0.335
4.114
1
0.043*
1.971
AF: atrial fibrillation/flutter; GDMT: guideline-directed medical therapy; PIM3: PIMs in older adults with caution; PIM4: drug-drug interactions; PIM5: PIMs based on renal function. *Factors with P-values less than 0.05.
Table
7.
Multiple logistic regression analysis of factors associated with cardiovascular readmission.
Variables
b
S.E.
Wals
df
Sig
OR
GDMT
0.552
0.273
4.074
1
0.044*
0.737
HF medications
0.243
0.125
3.780
1
0.052
1.274
Overall PIMs
0.179
0.099
3.250
1
0.071
1.196
PIM3
0.529
0.224
5.556
1
0.018*
1.697
No. diagnosed disease
0.096
0.076
1.589
1
0.207
1.101
BMI
−0.055
0.044
1.564
1
0.211
0.947
Coronary vascular disease
0.085
0.450
0.035
1
0.851
1.088
Hypertension
0.036
0.355
0.010
1
0.920
1.036
Diabetes
0.479
0.252
3.604
1
0.058
1.615
Myocardiopathy unknown origin
−1.083
0.623
3.020
1
0.082
0.339
Valvulopathy
−0.454
0.558
0.663
1
0.416
0.635
AF
0.797
0.374
4.546
1
0.033*
2.220
PVC/VT
−0.075
0.411
0.034
1
0.854
0.927
Cerebrovascular disease
0.184
0.415
0.197
1
0.657
1.202
Gastric or duodenal ulcers
−0.044
0.646
0.005
1
0.946
0.957
COPD/pulmonary infection
0.126
0.365
0.120
1
0.729
1.135
Cancer
−1.333
1.025
1.693
1
0.193
0.264
*Factors with P-values less than 0.05. AF: atrial fibrillation/flutter; BMI: body mass index; COPD: chronic obstructive pulmonary disease; GDMT: guideline-directed medical therapy; HF: heart failure; PIM3: PIMs in older adults with caution; PVC: premature ventricular contraction; VT: ventricular tachycardia.
Table
8.
Multiple logistic regression analysis of factors associated with cardiovascular death.
Variables
b
S.E.
Wals
df
Sig
OR
PIM5
1.415
0.574
6.083
1
0.014*
4.118
BMI
−0.155
0.092
2.849
1
0.091
0.856
Hypertension
0.160
0.774
0.043
1
0.836
1.174
Diabetes
−0.255
0.773
0.109
1
0.742
0.775
Valvulopathy
0.820
0.854
0.921
1
0.337
2.270
AF
1.505
0.778
3.745
1
0.053
4.503
PVC/VT
0.806
0.777
1.077
1
0.299
2.239
Cerebrovascular disease
1.637
0.779
4.420
1
0.036*
5.139
COPD/pulmonary infection
−0.063
0.821
0.006
1
0.939
0.939
*Factors with P-values less than 0.05. BMI: body mass index; PIM5: PIMs based on renal function; PVC: premature ventricular contraction; VT: ventricular tachycardia.


 DownLoad:
DownLoad: