Please cite this article as: GUO GG, LUO X, ZHU K, LI LL, OU YF. Fatal ventricular arrhythmias after osimertinib treatment for lung adenocarcinoma: a case report. J Geriatr Cardiol 2023; 20(3): 242−246. DOI: 10.26599/1671-5411.2023.03.009.
Citation:
Please cite this article as: GUO GG, LUO X, ZHU K, LI LL, OU YF. Fatal ventricular arrhythmias after osimertinib treatment for lung adenocarcinoma: a case report. J Geriatr Cardiol 2023; 20(3): 242−246. DOI: 10.26599/1671-5411.2023.03.009.
Please cite this article as: GUO GG, LUO X, ZHU K, LI LL, OU YF. Fatal ventricular arrhythmias after osimertinib treatment for lung adenocarcinoma: a case report. J Geriatr Cardiol 2023; 20(3): 242−246. DOI: 10.26599/1671-5411.2023.03.009.
Citation:
Please cite this article as: GUO GG, LUO X, ZHU K, LI LL, OU YF. Fatal ventricular arrhythmias after osimertinib treatment for lung adenocarcinoma: a case report. J Geriatr Cardiol 2023; 20(3): 242−246. DOI: 10.26599/1671-5411.2023.03.009.
Osimertinib, a third-generation epidermal growth factor receptor tyrosine kinase inhibitor (EGFR-TKIs), is approved globally as the first-line treatment for patients with EGFR mutations (EGFRm: Ex19del/L858R) and T790M resistance mutations in advanced non-small cell lung cancer (NSCLC).[1-3] With its widespread use, the cardiotoxicity of osimertinib has been of great concern. According to the U.S. Food and Drug Administration Adverse Events Reporting System (FAERS), the main cardiac-related adverse events with EGFR-TKIs are heart failure, QT prolongation, atrial fibrillation, acute myocardial infarction and pericardial effusion, and osimertinib has a higher incidence of QT prolongation, heart failure and atrial fibrillation than other EGFR-TKIs.[4] As mentioned in its package insert, a decline in left ventricular ejection fraction (LVEF) of > 10% from baseline and to less than 50% of LVEF occurred in 3.2% of patients following osimertinib treatment in clinical trials, 0.8% of patients were found to have a heart rate corrected QT interval (QTc) of > 500 ms, and 3.1% of patients had a QTc increase from baseline of > 60 ms. No QTc-related arrhythmias were reported.[5]
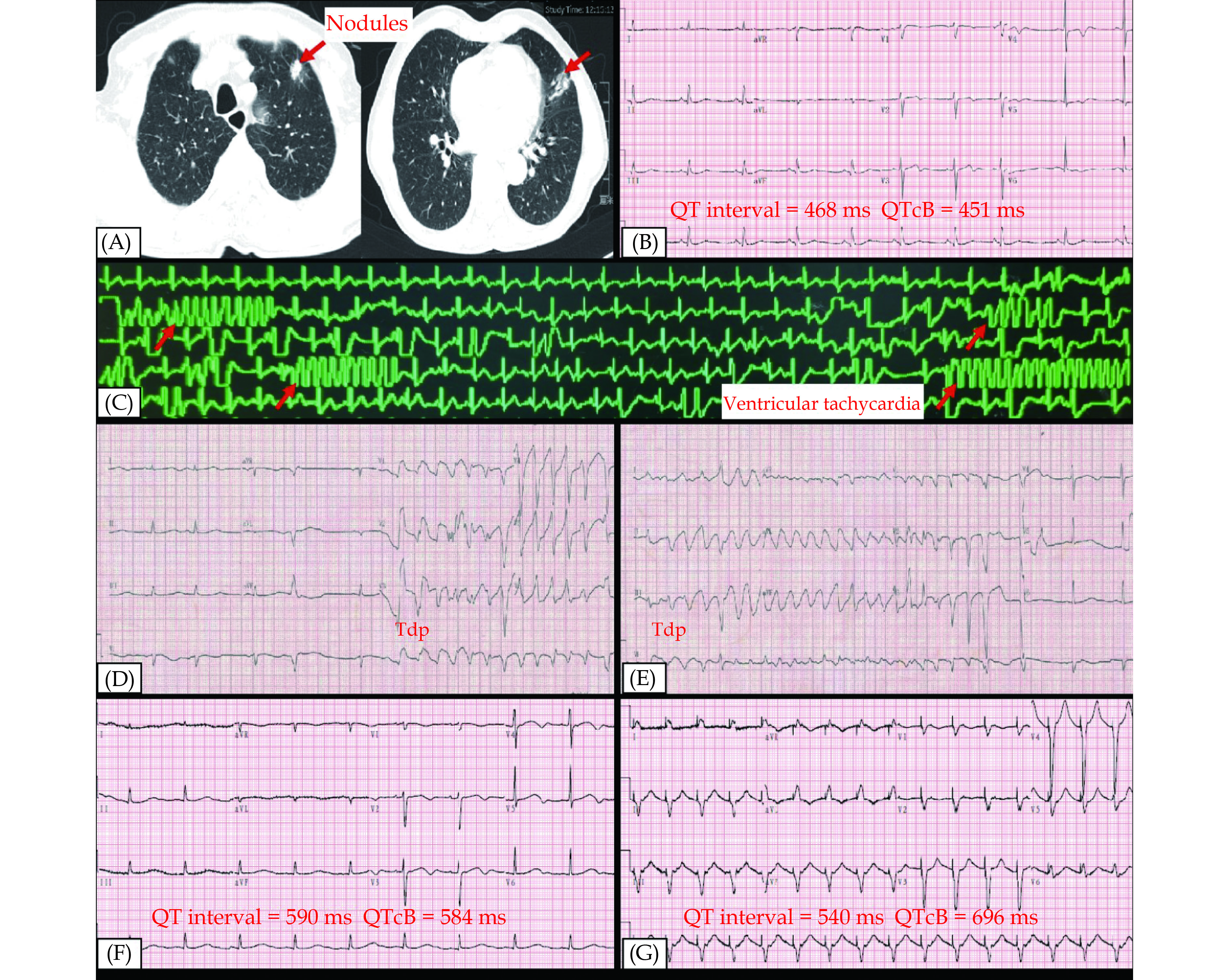
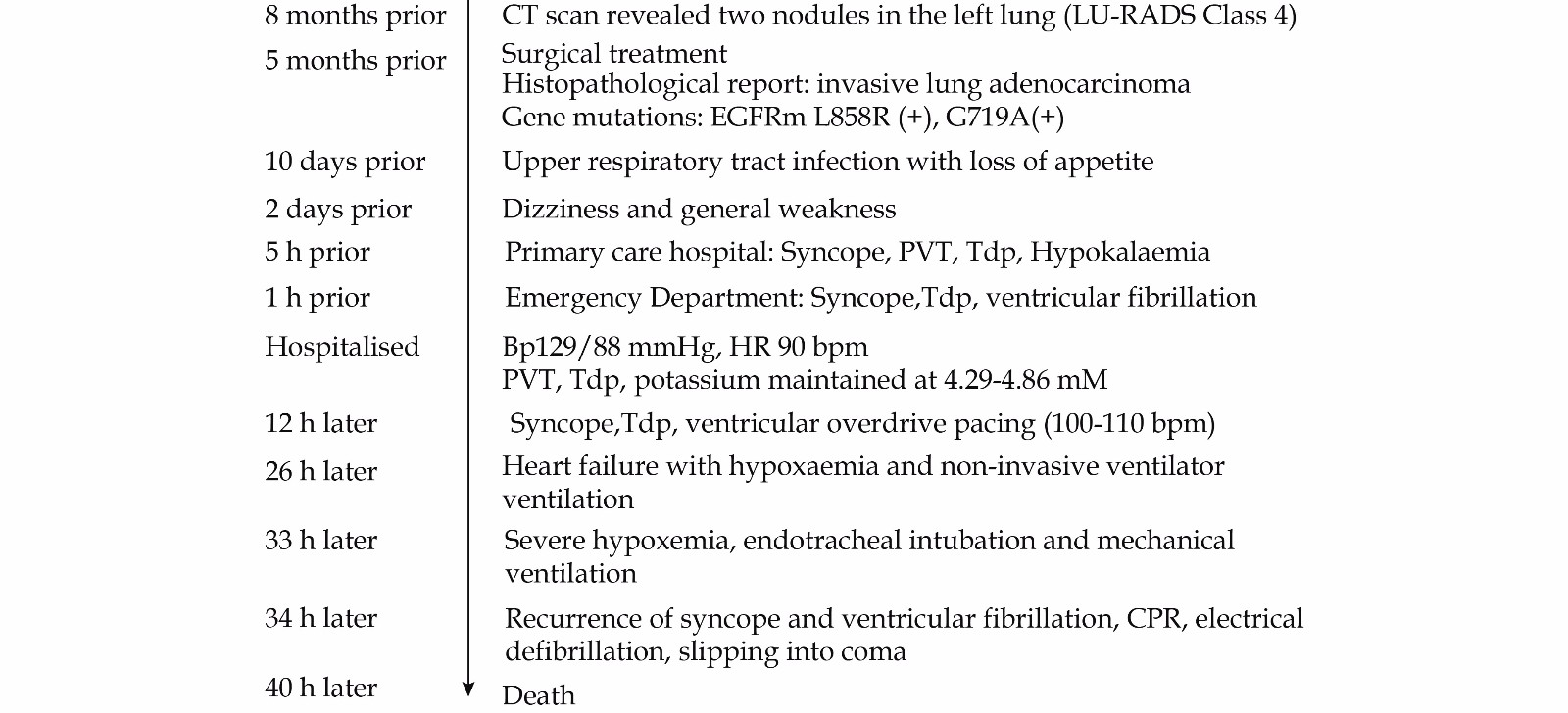
This is an 81-year-old male patient whose medical history is shown in Figure 1. Eight months ago, two nodules (LU-RADS class 4) in the left upper lung were revealed by CT scan at physical examination, located in the posterior apical segment and the lingual segment (Figure 2A). The patient presented with left-side chest pain and an electrocardiogram suggestive of lateral wall myocardial ischemia (Figure 2B). Accordingly, he underwent coronary angiography, the results of which showed 50% stenosis in the proximal segment of the left anterior descending branch, TIMI flow grade 3 distally and no significant stenosis in the rest of the coronary arteries. Severe coronary artery disease was ruled out and the chest pain was considered to be caused by a pulmonary nodule invading the pleura; therefore, he underwent thoracoscopic surgery for enlarged left upper lung resection five months ago. Histological sections of the resected nodules were taken for pathological and immunohistochemical examination, with the results suggesting that both nodules were invasive lung adenocarcinoma with EGFR (+). To guide the next treatment regimen, further detection of gene mutations in the histological sections was undertaken, with the results showing that EGFR mutations were in the lingual segment (L858R, Exon21) and the posterior apical segment (G719A, Exon18). Therefore, the patient started oral treatment with osimertinib at 80 mg once daily after discharge from the hospital. Prior, his electrocardiogram had suggested myocardial ischemia with a normal QT interval (QT/QTc interval 468/451 ms; Figure 2B), the ultrasonic cardiogram revealed that the atrial and ventricular size to be in the normal range, and LVEF was 60%.
Figure
1.
Medical history.
BP: blood pressure; BPM: beats per minute; CPR: cardiopulmonary resuscitation; CT: computer tomography; EGFRm: EGFR mutations; HR: heart rate; LU-RADS: lung reporting and data system; PVT: paroxysmal ventricular tachycardia; Tdp: torsades de pointes.
Ten days ago, due to an upper respiratory tract infection, the patient’s appetite decreased and his food intake was low. Two days ago, the patient experienced dizziness and general weakness but did not see a doctor at that time. The patient’s dizziness and weakness gradually worsened. Five hours ago, he was seen at a primary care hospital and collapsed with syncope while waiting in line; this lasted about two minutes and he regained consciousness without medical intervention. He was shortly thereafter admitted to the emergency resuscitation unit with a cardiac monitor. Frequent ventricular premature beats and paroxysmal ventricular tachycardia (PVT) could be seen on the cardiac monitor (Figure 2C). ECG was suggestive of torsades de pointes (Tdp) but of short duration, during which the patient did not lose consciousness (Figure 2D and E). Another ECG showed normal sinus rhythm and suggested QT prolongation (QT/QTc interval 590/584 ms; Figure 2F). Because of the presence of moderate hypokalaemia (2.65 mmol/L), the patient was treated with potassium chloride and magnesium sulphate supplementation, as well as intravenous anti-arrhythmic drugs such as lidocaine. During this period, the patient experienced a second loss of consciousness lasting less than one minute, when the cardiac monitor showed Tdp; this terminated spontaneously and he regained consciousness. For diagnosis and further treatment, the patient was transported to emergency department of Zhuzhou Hospital Affiliated to Xiangya School of Medicine. Shortly thereafter, he lost consciousness for the third time and the cardiac monitor showed ventricular fibrillation. Cardiopulmonary resuscitation (CPR) was immediately administered, after which the patient regained consciousness. He was then admitted immediately to the cardiac care unit (CCU), where 0.018 ng/mL troponin I (reference range 0.01–0.023 ng/mL) was detected. Potassium levels were maintained between 4.29–4.86 mmol/L and the cardiac monitor showed repeated PVT and Tdp. It was inferred that the ventricular arrhythmia may have been due to targeted agents and osimertinib was discontinued. To shorten the QT interval, a temporary pacemaker was placed for ventricular overdrive pacing (100–110 beats/min) and a repeat ECG showed a slight shortening of the QT interval (540 ms) but the QTc interval reached 696 ms (Figure 2G). Despite best efforts, the patient developed acute left heart failure (LVEF 30%) and severe hypoxaemia and there was no choice but to intubate and mechanically ventilate the patient. The patient again lost consciousness and developed ventricular fibrillation. Although resuscitated by up to 16 min of CPR and electric defibrillation to restore sinus rhythm, the patient developed irreversible brain damage into coma. The family refused advanced cardiopulmonary support such as extracorporeal membrane oxygenation (ECMO) and the patient subsequently died.
This is a case report of a male patient with advanced NSCLC who was treated with osimertinib after surgery. He was on the drug for five months without a dynamic ECG examination. At the time of medical consultation, there was recurrent syncope. ECG and the cardiac monitor suggested frequent ventricular premature beats, PVT and Tdp. The symptoms progressed rapidly and the patient soon developed fatal ventricular fibrillation, acute left heart failure, and eventually sudden cardiac death.
The human epidermal growth factor receptor family has four major members: EGFR (also known as HER1), HER2 (also known as ERBB2), ERBB3 (also known as HER3) and ERBB4 (also known as HER4). These regulate cell proliferation, survival, differentiation and migration through multiple intracellular signalling pathways. The human EGFR family plays an important role in the development and progression of tumours such as lung cancer and breast cancer.[6] EGFR mutation detection is recommended for all patients with advanced NSCLC to guide treatment.[7] Compared with conventional chemotherapy, EGFR-TKIs can improve progression-free survival in patients with advanced NSCLC.[8] Osimertinib is a third-generation EGFR-TKI that effectively, selectively and irreversibly inhibits both EGFR mutations (EGFRm: Ex19del/L858R) and T790M resistance mutations. Some studies have shown that osimertinib is more effective than other EGFR-TKIs in EGFR mutation–positive advanced NSCLC and has a similar safety profile and lower incidence of serious adverse events.[9,10]
Currently, osimertinib is widely used as adjuvant chemotherapy or combination chemotherapy after surgery for advanced NSCLC and its cardiotoxicity has been a hot topic of concern.[4,11-13] The results of the FLAURA phase 3 clinical study showed that QT interval prolongation was reported in a higher percentage of the osimertinib group than in the standard EGFR-TKI (gefitinib or erlotinib) group (10% vs. 4%) for patients with previously untreated, EGFR mutation–positive advanced NSCLC.[9] The incidence of heart failure was also higher (3.1% vs. 1.2%).[12] For the patients with T790M-positive advanced NSCLC, who had disease progression after other first-line EGFR-TKI therapies, the AURA phase 3 clinical study indicated that the incidence of QT interval prolongation and heart failure in the osimertinib group was 4% and 5%, respectively,[14] and no fatal ventricular arrhythmias occurred in these patients. There are some case reports of prolonged QT interval leading to PVT or Tdp after osimertinib treatment for advanced NSCLC; however, the basal rhythm could be restored without fatal consequences after rescue treatment, such as discontinuation of osimertinib, potassium and magnesium supplementation, ventricular overdrive pacing, and so on.[15-19]
To date, the underlying mechanism of osimertinib-induced cardiotoxicity is not fully understood. Cell repolarisation is mainly caused by potassium ion efflux and there are many different types of potassium ion channels on the cardiomyocyte membrane. Some studies have concluded that drug-induced QT interval prolongation is mainly due to the inhibition of potassium ion channels on the cardiomyocyte membrane.[20] Other studies have shown that EGFR-TKIs have a regulatory effect on potassium ion channels.[21-23] Additional findings have suggested that osimertinib has a weak inhibitory effect on the cardiac potassium ion channel Kv11.1, which is encoded by human ether-à-go-go-related gene (hERG) with an in vitro IC50 of 0.69 μm.[24] The spontaneous release of Ca2+ via cardiac ryanodine receptors (RyR2), through a process termed ‘store overload-induced Ca2+ release’ (SOICR), is a common mechanism underlying arrhythmia. It has been reported that silmitasertib and sunitinib can be assigned to their effect on RyR2 and increase in SOICR.[25] Osimertinib may have a similar effect but more research is needed to confirm this. Additionally, osimertinib can also have an inhibitory effect on HER2[26,27] and other HER2 inhibitors, such as trastuzumab, have a proven risk of cardiotoxicity.[28,29]
Notably, the patient had moderate hypokalaemia at the time of presentation. Hypokalaemia can prolong the QT interval and is a common pathogenesis of acquired long QT syndrome (LQTS), which can lead to Tdp. It has been shown that patients with EGFR mutation–positive advanced NSCLC who were treated with osimertinib could develop hypokalaemia.[30] Also, inadequate potassium intake is an important cause of hypokalaemia. In the present case, the patient had recurrent ventricular arrhythmias even after maintaining normal blood potassium stability. Therefore, it is speculated that hypokalaemia was not the root cause of this malignant arrhythmic event. Although an implantable cardioverter-defibrillator (ICD) is recommended for patients at high risk of LQTS, this would certainly have resulted in frequent electrical shocks for this patient and was therefore considered unsuitable. Additionally, because the patient was not followed up via regular ultrasonic cardiogram while on long-term osimertinib, the significant decline in LVEF during hospitalisation was presumed to be attributed to ventricular arrhythmias and it was not conclusive whether heart failure was osimertinib-induced.
The terminal half-life time of osimertinib is approximately 44 h, according to its package insert. Therefore, it must be discontinued once the QT interval is prolonged to more than 500 ms or ventricular arrhythmias occur. In this case, the disease progressed rapidly and, although the patient was also actively resuscitated—including by magnesium supplementation, application of antiarrhythmic drugs and maintenance of potassium stability—the treatment effect was poor. Even after placing a temporary pacemaker for ventricular overdrive pacing, the QTcB interval did not shorten and there was still repeated PVT and Tdp. The ultimate failure to save the patient’s life brought with it a profound lesson: although the probability of cardiovascular adverse events with osimertinib is extremely low, when it occurs, it can have serious, even life-threatening consequences. It is recommended that a full evaluation of cardiovascular risk factors via cardiac ultrasound, ECG, etc., be undertaken before the commencement of osimertinib treatment and that there be regular ECG review during the subsequent follow-up. In the case of QT interval prolongation combined with Tdp, polymorphic ventricular tachycardia and other symptoms of life-threatening arrhythmia, permanent discontinuation of osimertinib is required.
Ramalingam SS, Yang JC, Lee CK, et al. Osimertinib As First-Line Treatment of EGFR Mutation-Positive Advanced Non-Small-Cell Lung Cancer. J Clin Oncol 2018; 36: 841−849. doi: 10.1200/JCO.2017.74.7576
[2]
Yang JC, Ahn MJ, Kim DW, et al. Osimertinib in pretreated T790M-positive advanced non-small-cell lung cancer: AURA study phase II extension component. J Clin Oncol 2017; 35: 1288−1296. doi: 10.1200/JCO.2016.70.3223
[3]
John T, Akamatsu H, Delmonte A, et al. EGFR mutation analysis for prospective patient selection in AURA3 phase III trial of osimertinib versus platinum-pemetrexed in patients with EGFR T790M-positive advanced non-small-cell lung cancer. Lung Cancer 2018; 126: 133−138. doi: 10.1016/j.lungcan.2018.10.027
[4]
Anand K, Ensor J, Trachtenberg B, Bernicker EH. Osimertinib-Induced Cardiotoxicity: A Retrospective Review of the FDA Adverse Events Reporting System (FAERS). JACC Cardio Oncol 2019; 1: 172−178. doi: 10.1016/j.jaccao.2019.10.006
[5]
Pharmaceuticals A. Tagrisso (osimertinib) [package insert]. U. S. Food and Drug Administration website. Revised: September 2022. https://www.drugs.com/pro/tagrisso.html#s-34067-9 (accessed on October 8, 2022).
[6]
Yu J, Fang T, Yun C, et al. Antibody-drug conjugates targeting the human epidermal growth factor receptor family in cancers. Front Mol Biosci 2022; 9: 847835. doi: 10.3389/fmolb.2022.847835
[7]
Lindeman NI, Cagle PT, Aisner DL, et al. Updated molecular testing guideline for the selection of lung cancer patients for treatment with targeted tyrosine kinase inhibitors: guideline from the college of american pathologists, the international association for the study of lung cancer, and the association for molecular pathology. J Mol Diagn 2018; 20: 129−159. doi: 10.1016/j.jmoldx.2017.11.004
[8]
Ma H, Tian X, Zeng XT, et al. The efficacy of erlotinib versus conventional chemotherapy for advanced nonsmall-cell lung cancer: a PRISMA-compliant systematic review with meta-regression and meta-analysis. Medicine (Baltimore) 2016; 95: e2495. doi: 10.1097/MD.0000000000002495
[9]
Soria JC, Ohe Y, Vansteenkiste J, et al. Osimertinib in untreated EGFR-mutated advanced non-small-cell lung cancer. N Engl J Med 2018; 378: 113−125. doi: 10.1056/NEJMoa1713137
[10]
Ramalingam SS, Vansteenkiste J, Planchard D, et al. Overall survival with osimertinib in untreated, EGFR-mutated advanced NSCLC. N Engl J Med 2020; 382: 41−50. doi: 10.1056/NEJMoa1913662
[11]
Kunimasa K, Kamada R, Oka T, et al. Cardiac adverse events in EGFR-mutated non-small cell lung cancer treated with osimertinib. JACC Cardio Oncol 2020; 2: 1−10. doi: 10.1016/j.jaccao.2020.02.003
[12]
Ewer MS, Tekumalla SH, Walding A, Atuah KN. Cardiac safety of osimertinib: a review of data. J Clin Oncol 2021; 39: 328−337.
[13]
Kunimasa K. Is osimertinib-induced cardiotoxicity really harmless? J Clin Oncol 2021; 39: 2050-2051.
[14]
Mok TS, Wu YL, Ahn MJ, et al. Osimertinib or platinum-pemetrexed in EGFR T790M-positive lung cancer. N Engl J Med 2017; 376: 629−640. doi: 10.1056/NEJMoa1612674
[15]
Matsuura C, Kato T, Koyama K. Successful management of refractory torsades de pointes due to drug-induced long QT syndrome guided by point-of-care monitoring of ionized magnesium. Cureus 2021; 13: e13939.
[16]
Ikebe S, Amiya R, Minami S, et al. Osimertinib-induced cardiac failure with QT prolongation and torsade de pointes in a patient with advanced pulmonary adenocarcinoma. Int Cancer Conf J 2021; 10: 68−71. doi: 10.1007/s13691-020-00450-2
[17]
Bian S, Tang X, Lei W. A case of torsades de pointes induced by the third-generation EGFR-TKI, osimertinib combined with moxifloxacin. BMC Pulm Med 2020; 20: 181. doi: 10.1186/s12890-020-01217-4
[18]
Kaira K, Ogiwara Y, Naruse I. Occurrence of ventricular fibrillation in a patient with lung cancer receiving osimertinib. J Thorac Oncol 2020; 15: e54−e55. doi: 10.1016/j.jtho.2019.11.029
[19]
Zhang Y, Wang X, Pan Y, et al. Overdrive pacing in the acute management of osimertinib-induced ventricular arrhythmias: A case report and literature review. Front Cardiovasc Med 2022; 9: 934214. doi: 10.3389/fcvm.2022.934214
[20]
Li S, Xu Z, Guo M, et al. Drug-induced QT Prolongation Atlas (DIQTA) for enhancing cardiotoxicity management. Drug Discov Today 2022; 27: 831−837. doi: 10.1016/j.drudis.2021.10.009
[21]
Garcia-Quiroz J, Gonzalez-Gonzalez ME, Diaz L, et al. Astemizole, an Inhibitor of Ether-a-Go-Go-1 potassium channel, increases the activity of the tyrosine kinase inhibitor gefitinib in breast cancer cells. Rev Invest Clin 2019; 71: 186−194.
[22]
Teisseyre A, Palko-Labuz A, Sroda-Pomianek K, Michalak K. Voltage-gated potassium channel Kv1.3 as a target in therapy of cancer. Front Oncol 2019; 9: 933.
[23]
Aissaoui D, Mlayah-Bellalouna S, Jebali J, et al. Functional role of Kv1.1 and Kv1. 3 channels in the neoplastic progression steps of three cancer cell lines, elucidated by scorpion peptides. Int J Biol Macromol 2018; 111: 1146−1155.
[24]
Jin T, Hu B, Chen S, et al. An in vitro assay of hERG K (+) channel potency for a new EGFR inhibitor FHND004. Front Pharmacol 2018; 9: 577. doi: 10.3389/fphar.2018.00577
[25]
Chakraborty AD, Gonano LA, Munro ML, et al. Activation of RyR2 by class I kinase inhibitors. Br J Pharmacol 2019; 176: 773−786. doi: 10.1111/bph.14562
[26]
Liu S, Li S, Hai J, et al. Targeting HER2 aberrations in non-small cell lung cancer with osimertinib. Clin Cancer Res 2018; 24: 2594−2604. doi: 10.1158/1078-0432.CCR-17-1875
[27]
Das D, Xie L, Wang J, et al. In vivo efficacy studies of novel quinazoline derivatives as irreversible dual EGFR/HER2 inhibitors, in lung cancer xenografts (NCI-H1975) mice models. Bioorg Chem 2020; 99: 103790. doi: 10.1016/j.bioorg.2020.103790
[28]
Nicolazzi MA, Carnicelli A, Fuorlo M, et al. Anthracycline and trastuzumab-induced cardiotoxicity in breast cancer. Eur Rev Med Pharmacol Sci 2018; 22: 2175−2185.
[29]
Dempsey N, Rosenthal A, Dabas N, et al. Trastuzumab-induced cardiotoxicity: a review of clinical risk factors, pharmacologic prevention, and cardiotoxicity of other HER2-directed therapies. Breast Cancer Res Treat 2021; 188: 21−36. doi: 10.1007/s10549-021-06280-x
[30]
Chihara Y, Takeda T, Goto Y, et al. A phase II trial on osimertinib as a first-line treatment for EGFR mutation-positive advanced NSCLC in elderly patients: The SPIRAL-0 Study. Oncologist 2022; 27: e834−e903.


 DownLoad:
DownLoad: