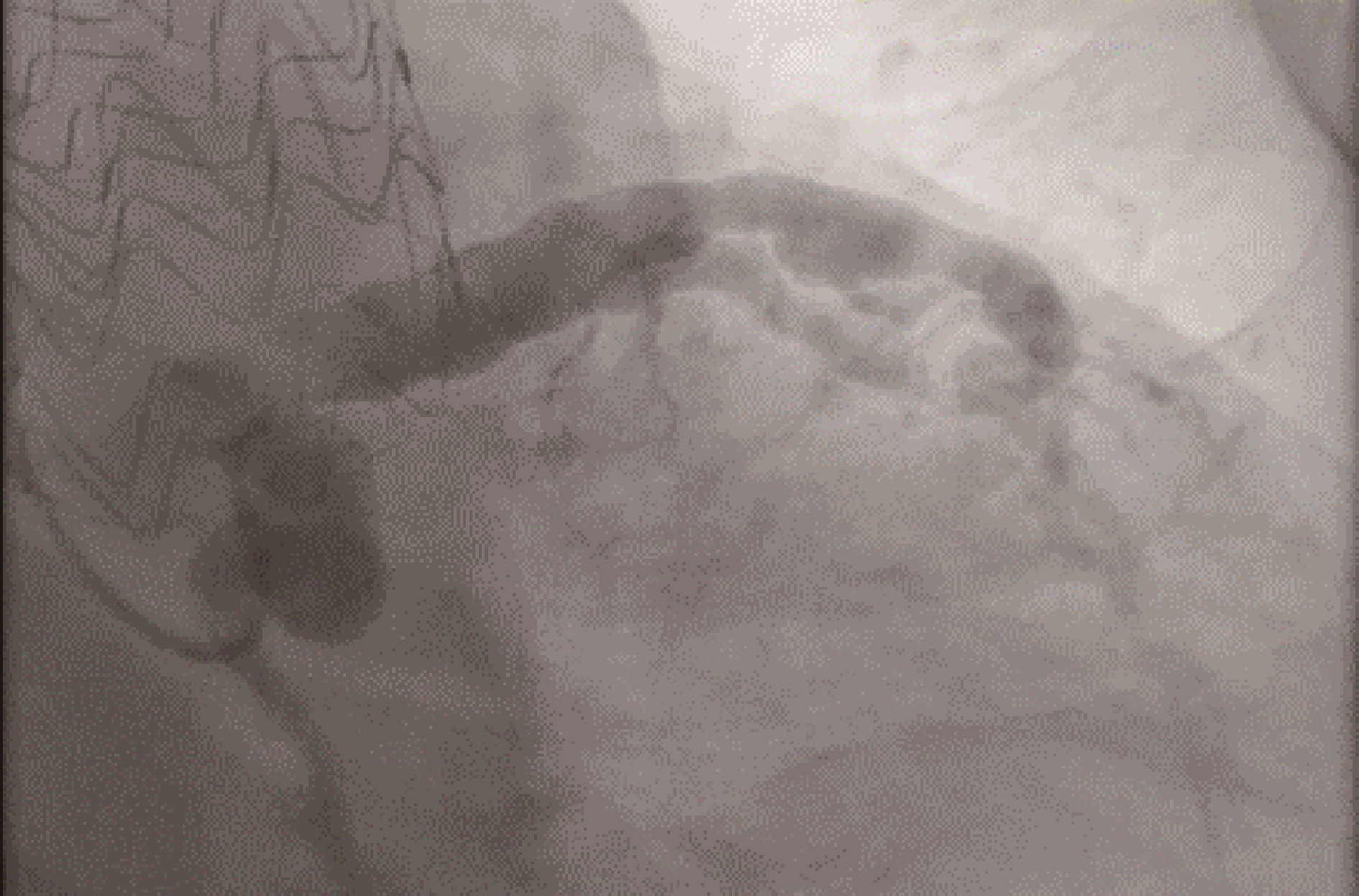
A 64-year-old male with a history of thoracic aortic ulcer s/p thoracic endovascular aortic repair presented to the hospital with typical chest pain. His initial physical exam was unremarkable. Cardiac biomarkers were negative on admission and electrolytes were within normal limits. Telemetry revealed a wide complex tachycardia, with 12-lead electrocardiogram confirming ventricular tachycardia. Subsequently, the patient became unstable resulting in direct current cardioversion (DCCV). He subsequently reverted back into ventricular tachycardia requiring additional DCCV, and was then placed on an amiodarone infusion. He underwent emergent left heart catheterization which revealed severe coronary ectasia of the left anterior descending coronary artery and left circumflex coronary artery (Figure 1). Right coronary artery showed severe ectasia with a possible thrombosis distally (Figure 2). Given the patient diffuse and severe disease, percutaneous coronary intervention was not preformed and instead he was evaluated by cardiothroacic surgery. Transthoracic echocardiogram revealed an ejection fraction of 45% with global hypokinesis. Cardiac magnetic resonance imaging showed scarring of the basal and mid inferior lateral wall. Rheumatological workup to elucidate any underlying connective tissue disorders was unrevealing. The patient underwent successful five vessel coronary artery bypass grafting and made a full recovery.
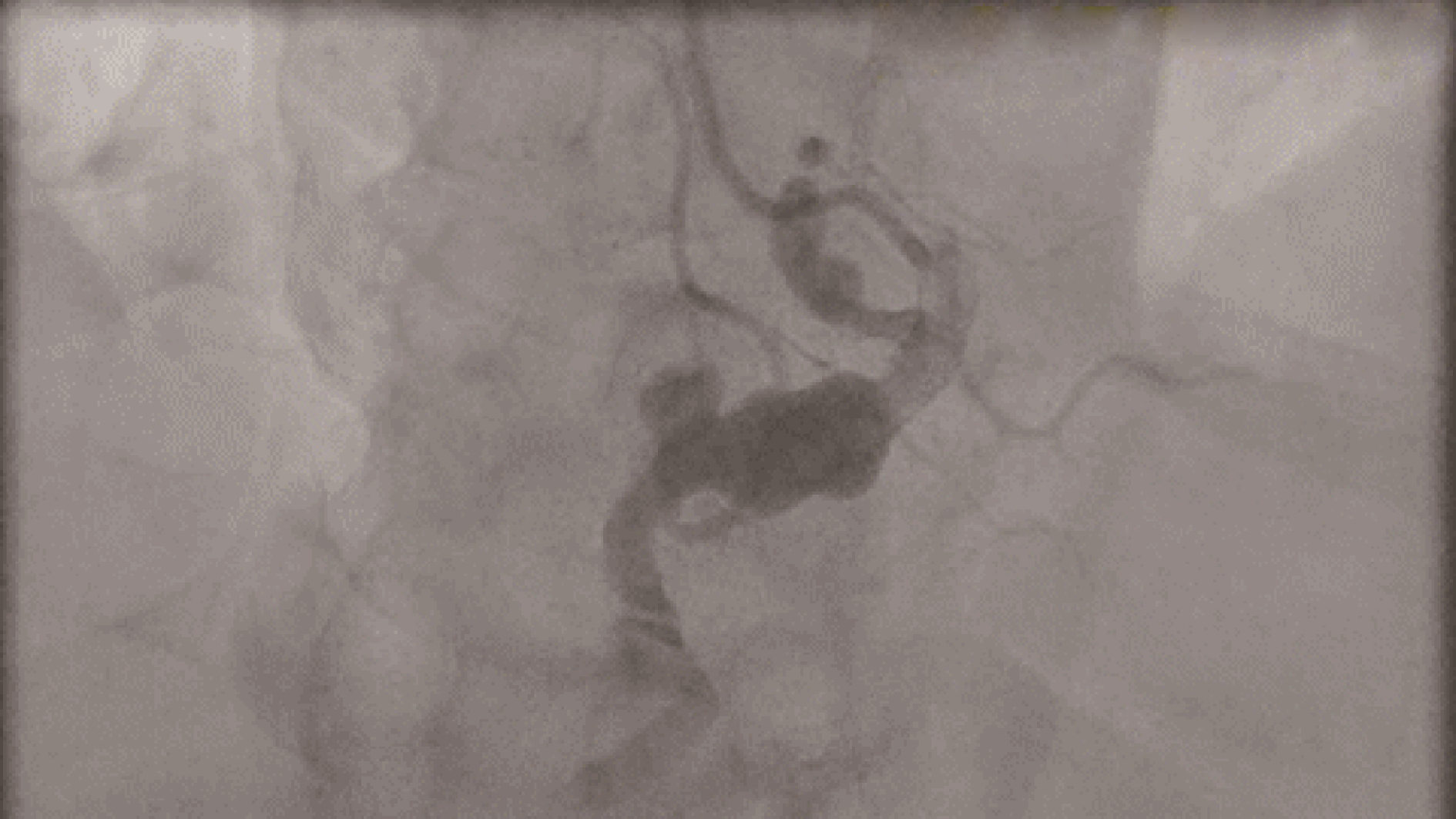
Figure
1.
Left heart catheterization: left anterior oblique caudal view.
Severe coronary ectasia of the left anterior descending coronary artery and left circumflex coronary artery.
Coronary artery ectasia (CAE) is characterized by the aneurismal dilation of the coronary arteries with a diameter 1.5 times the adjacent normal coronary artery based on Coronary Artery Surgery Study registry.[1] It is a rare condition with an incidence of 1.4%-4.9%.[1] CAE differs from coronary artery aneurisms as the former usually involves multiple or diffuse involvement of coronary arteries.[1] Although CAE is well described, the underlying pathophysiology is not well understood. There are multiple etiologies of this condition, the most common being atherosclerosis.[2]
Atherosclerosis typically causes narrowing of the vessel lumen, however in ectasia luminal dilation due to arterial remodeling of certain plaques results in expansion of the media and external elastic membrane.[3] In addition to atherosclerosis, other common etiologies include vasculitis (Kawasaki), connective tissue disease, systemic infections, drugs, and genetic abnormalities.[3]
Most cases are discovered incidentally via angiography, [3] however it often presents as acute coronary syndrome (ACS). This occurs because of diminished coronary flow, or stagnancy of blood flow causing formation of intracoronary thrombus with embolization distally.[3] Aneurysmal rupture can also occur which can lead to tamponade or fistula formation.[3] Coronary angiography is the gold standard for diagnosing these patients. In this particular case, the patient had diffuse disease causing ischemia which lead to scarring of the myocardium. This lead to recurrent ventricular tachycardia which is an unusual presentation of CAE.
Given the lack of randomized trials, treatment for these patients vary.[3] Because atherosclerosis is implicated in the causation of most cases of CAE, aggressive risk factor modification is key.[2, 3] Some studies also show some benefit using additional antiplatelet medications or anticoagulation in very high risk patients. Percutaneous coronary intervention can be considered and has shown benefits in cases with ACS, however studies are limited. Surgery remains the first line therapy for patients, especially ones with involvement of the left main and/or severe disease.[1] Long-term prognosis in patients with CAE is unknown. In the Coronary Artery Surgery Study registry, no difference in survival was observed between patients with or without CAE.[1] Several studies thereafter failed to show a mortality difference between CAE and coronary artery disease and concluded that CAE is a variant of atherosclerosis that confers no additional risk.[1] However, more recent studies have suggested that the presence of CAE especially in patients with ACS was predictive of future myocardial infarction and possible cardiac death.[4] This makes it clear that further study of this disease process is essential for future management.
Coronary artery ectasia is a very rare clinical entity that can present a variety of ways including angina, ACS, tamponade, incidentally, or with ventricular tachycardia as in this case. Coronary angiogphrapy is the gold standard in diagnosing these patients, and is important to understand the image findings, disease process, and classifications to ensure accurate diagnosis. Further studies into this disease process are essential in order to develop more uniform treatment strategies and determine long-term prognosis for these patients.


 DownLoad:
DownLoad: