Please cite this article as: FAN HL, ZENG LH, CHEN PY, LIU YH, DUAN CY, HE WF, TAN N, CHEN JY, HE PC. Association of baseline hemoglobin A1c levels with bleeding in patients with non-ST-segment elevation acute coronary syndrome underwent percutaneous coronary intervention: insights of a multicenter cohort study from China. J Geriatr Cardiol 2022; 19(7): 487−497. DOI: 10.11909/j.issn.1671-5411.2022.07.004.
Citation:
Please cite this article as: FAN HL, ZENG LH, CHEN PY, LIU YH, DUAN CY, HE WF, TAN N, CHEN JY, HE PC. Association of baseline hemoglobin A1c levels with bleeding in patients with non-ST-segment elevation acute coronary syndrome underwent percutaneous coronary intervention: insights of a multicenter cohort study from China. J Geriatr Cardiol 2022; 19(7): 487−497. DOI: 10.11909/j.issn.1671-5411.2022.07.004.
Please cite this article as: FAN HL, ZENG LH, CHEN PY, LIU YH, DUAN CY, HE WF, TAN N, CHEN JY, HE PC. Association of baseline hemoglobin A1c levels with bleeding in patients with non-ST-segment elevation acute coronary syndrome underwent percutaneous coronary intervention: insights of a multicenter cohort study from China. J Geriatr Cardiol 2022; 19(7): 487−497. DOI: 10.11909/j.issn.1671-5411.2022.07.004.
Citation:
Please cite this article as: FAN HL, ZENG LH, CHEN PY, LIU YH, DUAN CY, HE WF, TAN N, CHEN JY, HE PC. Association of baseline hemoglobin A1c levels with bleeding in patients with non-ST-segment elevation acute coronary syndrome underwent percutaneous coronary intervention: insights of a multicenter cohort study from China. J Geriatr Cardiol 2022; 19(7): 487−497. DOI: 10.11909/j.issn.1671-5411.2022.07.004.
Association of baseline hemoglobin A1c levels with bleeding in patients with non-ST-segment elevation acute coronary syndrome underwent percutaneous coronary intervention: insights of a multicenter cohort study from China
Department of Cardiology, School of Medicine, South China University of Technology, Guangzhou, China
2.
Department of Cardiology, Guangdong Cardiovascular Institute, Guangdong Provincial People’s Hospital, Guangdong Academy of Medical Sciences, Guangzhou, China
3.
Guangdong Provincial Key Laboratory of Coronary Heart Disease Prevention, Guangdong Provincial People’s Hospital, Guangdong Academy of Medical Sciences, Guangzhou, China
4.
The Second School of Clinical Medicine, Southern Medical University, Guangzhou, China
5.
Department of Cardiology, the Second People’s Hospital of Nanhai District, Guangdong Provincial People’s Hospital’s Nanhai Hospital, Foshan, China
6.
Department of Biostatistics, School of Public Health, Southern Medical University, Guangzhou, China
7.
Department of Cardiology, Heyuan People’s Hospital, Heyuan, China
OBJECTIVE To investigate the association between baseline hemoglobin A1c (HbA1c) levels and bleeding in patients with non-ST-segment elevation acute coronary syndrome (NSTE-ACS) who underwent percutaneous coronary intervention (PCI).
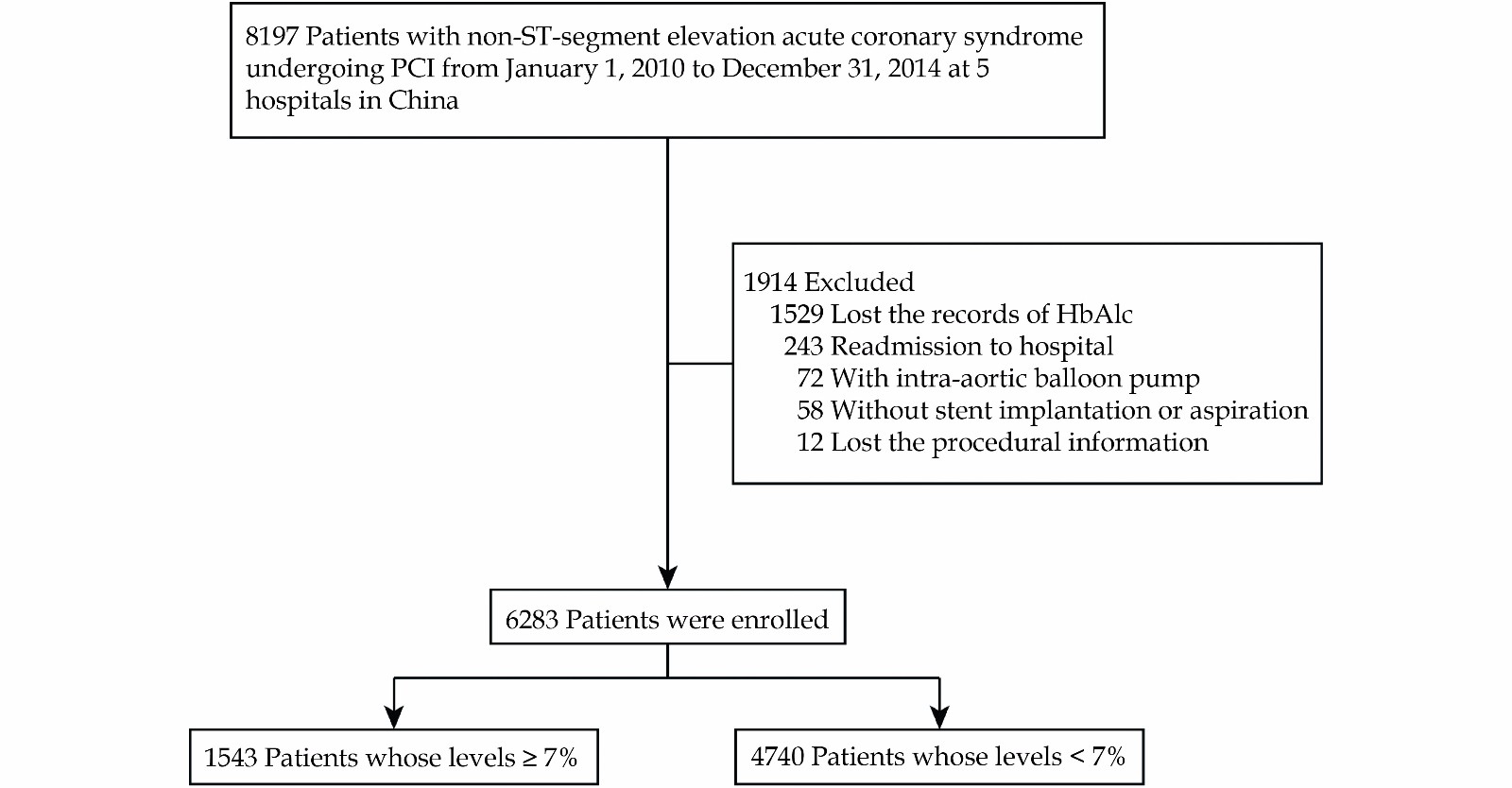
METHODS This observational cohort study enrolled 6283 consecutive NSTE-ACS patients undergoing PCI from January 1, 2010 to December 31, 2014. Based on baseline HbA1c levels, the patients were divided into the group with HbA1c < 7% (n = 4740) and the group with HbA1c ≥ 7% (n = 1543). The primary outcomes are major bleeding (BARC grades 3-5) and all-cause death during follow-up.
RESULTS Of patients enrolled, 4705 (74.9%) were male, and 2143 (34.1%) had a history of diabetes mellitus, with a mean (SD) age of 64.13 (10.32) years. The median follow-up duration was 3.21 years. Compared with the patients with HbA1c < 7%, the risk of major bleeding events during follow-up was higher in patients with HbA1c ≥ 7% (adjusted hazard ratio [HR] = 1.57; 95% confidence interval [CI]: 1.01-2.44; P = 0.044), while the risk of all-cause death during follow-up was not associated with the higher HbA1c levels (adjusted HR = 0.88; 95% CI: 0.66-1.18; P = 0.398).
CONCLUSIONS Compared with the lower baseline HbA1c levels, the higher baseline HbA1c levels were associated with an increase in long-term bleeding risk in NSTE-ACS patients undergoing PCI, though higher baseline HbA1c levels were not associated with the higher risk in all-cause death.
Diabetes mellitus (DM) is associated with a higher risk of ischemia events, including mortality, heart failure, and stroke, in patients with non-ST-segment elevation acute coronary syndrome (NSTE-ACS).[1-3] Noticeably, patients with NSTE-ACS and DM had the worst long-term prognosis among all ACS patients.[4] Additionally, DM has been determined as the independent predictor of in-hospital bleeding events in patients with non-ST-segment elevation myocardial infarction (NSTEMI).[5,6] Although dual antiplatelet therapy (DAPT) has been identified as the core component of management of NSTE-ACS, no specific recommendation on antithrombotic pharmacotherapy for NSTE-ACS patients with DM has been made.[7,8] Thus, the optimal prediction for the prognosis of patients with NSTE-ACS is important.
Since the history of DM has been identified as the independent predictive factor for bleeding events in patients with NSTEMI,[5] HbA1c levels may be a predictive factor of bleeding in ACS patients undergoing percutaneous coronary intervention (PCI). A recent study has demonstrated that the association between baseline HbA1c levels and all-cause death or myocardial infarction in patients with ACS displays U-shape curve.[9]
The previous study has reported that higher HbA1c levels were associated with a higher incidence of bleeding events in ACS patients, including those who received invasive treatment or only medical management.[10] NSTE-ACS patients undergoing PCI who were administrated with additional anticoagulants during procedure had a higher risk of bleeding events.[11,12] Thus, the association between baseline HbA1c levels and bleeding events in NSTE-ACS patients undergoing PCI should be further investigated.
METHODS
Study Design and Population
Based on our previously published multicenter cohort study,[13] this observational cohort study enrolled 8197 consecutive NSTE-ACS patients undergoing PCI from January 1, 2010 to December 31, 2014 at five centers in China. The study protocol was approved by the central ethics committee of the Guangdong Provincial People’s Hospital, Guangzhou, China, with a waiver of informed consent (No. GDREC2016210H(R1)). Central ethical approval was applicable at the other collaborating hospitals as well. The patients above 18 years and had information about the history of T2DM and admission HbA1c were enrolled. Patients were excluded if they required an intra-aortic balloon pump, did not receive stent implantation or aspiration, were readmitted to the hospital, and their information on PCI procedure was missed. Finally, 6283 patients were included in this study. Based on baseline HbA1c levels, the patients were divided into the HbA1c < 7% group and the HbA1c ≥ 7% group (Figure 1).
Data including patient demographics, laboratory test results, PCI procedural details, antithrombotic therapies, other medical treatments, and clinical events were extracted from the hospital electrical records by investigators. Follow-up was conducted by trained nurses via telephone interviews or clinical visits.
Outcomes
The primary outcomes were major bleeding and all-cause death during follow-up. The secondary outcomes included several in-hospital events, including all-cause death, major bleeding, any bleeding, and major adverse cardiovascular events (MACEs). The secondary outcomes also included any bleeding during follow-up.
Major bleeding and any bleeding were defined by the BARC grades 3-5 and grades 1-5,[14] respectively. MACEs were defined as the composite events of all-cause death, myocardial infarction, target vessel revascularization, and stroke.
Statistical Analyses
Continuous variables following normal distribution were presented as mean ± SD, and the differences between groups were analyzed using two-sample t-tests. Non-normally distributed continuous variables were expressed as medians and interquartile ranges and were compared using Wilcoxon rank-sum tests. Categorical variables were described as a number (n) with percentage (%), and differences were analyzed by Pearson χ2 or Fisher exact test.
Logistic regression was performed as a multivariable analysis for in-hospital outcomes. Cox proportional hazards regression model was performed as a multivariable analysis for clinical outcomes during follow-up. An additive hazards model was used to detect time-varying associations. Potential confounders that were significant in the univariate analysis or clinically important. Age, sex, heart rate, systolic blood pressure, hemoglobin levels, history of DM, history of myocardial infarction, history of PCI, history of hypertension, current smoking, estimated glomerular filtration rate (eGFR), DAPT, glycoprotein Ⅱb/Ⅲa inhibitor, warfarin, parenteral anticoagulation therapy, the diagnosis of NSTE-ACS subtypes were adjusted in the multivariable models for bleeding events in hospital and during follow-up.
For adjustment of logistic regression analyses for in-hospital death and in-hospital MACEs, age, sex, history of myocardial infarction, history of stroke, chronic heart failure, eGFR, diagnosis of NSTE-ACS subtypes, coronary anatomy, the interval from admission to PCI procedure were included. For adjustment of all-cause death during follow-up, age, sex, heart rate, systolic blood pressure, left ventricular ejection fraction (LVEF), history of DM, history of myocardial infarction, history of PCI, history of hypertension, current smoking, eGFR, DAPT, glycoprotein Ⅱb/Ⅲa inhibitor, angiotensin converting enzyme inhibitors/angiotensin receptor blockers (ACEI/ARB), parenteral anticoagulation therapy, coronary anatomy, implanted stents number, total implanted stents length, the diagnosis of NSTE-ACS subtypes, and the interval from admission to PCI procedure were included in multivariable analyses.
Subgroup analyses were conducted for major bleeding during follow-up. For each outcome, the most clinically relevant subgroups were analyzed. For each subgroup, the multivariable analysis was performed by adjusting all other subgroup factors. Forest plots were used to show the results.
All analyses were performed with SAS version 9.4 (SAS Institute, Cary, NC). All significant interactions were also examined. A two-sided P < 0.05 was considered statistically significant.
RESULTS
Baseline Characteristics
Of 6283 patients enrolled, 4705 (74.9%) were male, and 2143 (34.1%) had a history of T2DM, with a mean age of 64.13 ± 10.32 years. The median follow-up duration was 3.21 years. Among these patients, 3497 were diagnosed with NSTEMI (55.7%), and 2786 were diagnosed with unstable angina (44.3%). Based on baseline HbA1c levels, 4740 patients had the levels of admission HbA1c < 7%, and 1543 patients had the levels of admission HbA1c ≥ 7%. Patients with baseline HbA1c levels ≥ 7% were older and more likely to have higher heart rate, systolic blood pressure, serum creatinine levels, history of T2DM, and chronic heart failure than those with baseline HbA1c levels < 7%. Additionally, those with baseline HbA1c levels ≥ 7% had lower hematocrit and eGFR. Among patients with baseline HbA1c levels ≥ 7%, 1365 were diagnosed with T2DM, and 30.1% were administrated insulin. In patients with baseline HbA1c levels < 7%, 778 patients had T2DM, and 1.8% received insulin (Table 1).
Table
1.
Characteristics of patients at index hospitalization according to HbA1c levels.
Characteristics
HbA1c ≥ 7% (n = 1543)
HbA1c < 7% (n = 4740)
Total (n = 6283)
P-value
Age
Mean, yrs
64.72 ± 9.73
63.93 ± 10.50
64.13 ± 10.32
0.007
≥ 65 yrs,
806 (52.2%)
2343 (49.4%)
3149 (50.1%)
0.056
Female
471 (30.5%)
1107 (23.4%)
1578 (25.1%)
< 0.001
Weight, kg
67.79 ± 12.21
65.89 ± 11.77
66.36 ± 11.90
< 0.001
Heart rate, beats/min
75.72 ± 11.96
73.13 ± 11.33
73.77 ± 11.54
< 0.001
Blood pressure, mmHg
Systolic
136.70 ± 19.63
133.89 ± 19.59
134.58 ± 19.64
< 0.001
Diastolic
77.58 ± 11.54
77.63 ± 11.74
77.62 ± 11.69
0.873
LVEF, %
60.39% ± 10.92%
62.19% ± 9.65%
61.75% ± 10.01%
< 0.001
History of disease and risk factors
Myocardial infarction
263 (17.0%)
710 (15.0%)
973 (15.5%)
0.051
PCI
332 (21.5%)
758 (16.0%)
1090 (17.3%)
< 0.001
CABG
20 (1.3%)
49 (1.0%)
69 (1.1%)
0.390
Stroke
116 (7.5%)
338 (7.1%)
454 (7.2%)
0.610
Chronic heart failure
237 (15.4%)
578 (12.2%)
815 (13.0%)
0.001
Atrial fibrillation
55 (3.6%)
157 (3.3%)
212 (3.4%)
0.634
Current smoker
372 (24.1%)
1412 (29.8%)
1784 (28.4%)
< 0.001
Diabetes mellitus
1365 (88.5%)
778 (16.4%)
2143 (34.1%)
< 0.001
Hypertension
1142 (74.0%)
3107 (65.5%)
4249 (67.6%)
< 0.001
Hyperlipemia
339 (22.0%)
1062 (22.4%)
1401 (22.3%)
0.722
eGFR
Mean, mL/min per 1.73 m2
80.94 ± 28.33
83.19 ± 24.19
82.64 ± 25.29
0.005
≤ 60 mL/min per 1.73 m2
357 (23.1%)
699 (14.7%)
1056 (16.8%)
< 0.001
Serum creatinine level, mg/dL
1.07 ± 0.70
1.02 ± 0.63
1.03 ± 0.65
0.017
Anemia
531 (34.4%)
1401 (29.6%)
1932 (30.7%)
< 0.001
Haemoglobin, g/L
132.00 ± 17.51
134.42 ± 16.45
133.82 ± 16.75
< 0.001
Type of disease,
NSTEMI
677 (43.9%)
2109 (44.5%)
2786 (44.3%)
0.671
UA
866 (56.1%)
2631 (55.5%)
3497 (55.7%)
In-hospital medication
Aspirin
1503 (97.4%)
4631 (97.7%)
6134 (97.6%)
0.431
Clopidogrel
1530 (99.2%)
4699 (99.1%)
6229 (99.1%)
0.007
Ticagrelor
3 (0.2%)
8 (0.2%)
11 (0.2%)
0.044
Dual antiplatelet therapy
1496 (97.0%)
4604 (97.1%)
6100 (97.1%)
0.720
Statin
1511 (97.9%)
4648 (98.1%)
6159 (98.0%)
0.744
Warfarin
13 (0.8%)
20 (0.4%)
33 (0.5%)
0.047
ACEI/ARB
1270 (82.3%)
3655 (77.1%)
4925 (78.4%)
< 0.001
Beta blockers
1300 (84.3%)
3961 (83.6%)
5261 (83.7%)
0.526
Parenteral anticoagulation therapy
592 (38.4%)
1895 (40.0%)
2487 (39.6%)
0.261
Glycoprotein IIb/IIIa inhibitor
186 (12.1%)
525 (11.1%)
711 (11.3%)
0.292
Hypoglycemic therapy
Insulin
322 (30.1%)
58 (1.8%)
380 (9.0%)
< 0.001
hypoglycemic drugs
748 (70.0%)
358 (11.3%)
1106 (26.1%)
< 0.001
Positive cardiac biomarkers
820 (55.2%)
2460 (53.7%)
3280 (54.1%)
0.315
Procedure characteristics
Access site
Transradial access
1312 (85.0%)
4076 (86.0%)
5388 (85.8%)
0.347
Transfemoral access
231 (15.0%)
664 (14.0%)
895 (14.2%)
Coronary anatomy
Left main
188 (12.2%)
576 (12.2%)
764 (12.2%)
Multivessel disease
1077 (69.8%)
2928 (61.8%)
4005 (63.7%)
< 0.001
Other
278 (18.0%)
1236 (26.1%)
1514 (24.1%)
Stents number
2.13 ± 1.22
1.99 ± 1.14
2.02 ± 1.16
< 0.001
Total length of stents, mm
46 (28-72)
42 (24-66)
42 (24-68)
< 0.001
Interval between admission and procedure
Median, days
2 (1-4)
2 (1-3)
2 (1-4)
0.021
< 24 h
628 (40.7%)
2064 (43.5%)
2692 (42.8%)
24-72 h
500 (32.4%)
1497 (31.6%)
1997 (31.8%)
0.115
> 72 h
415 (26.9%)
1179 (24.9%)
1594 (25.4%)
Data are presented as n (%) or median (IQR). ACEI: angiotensin converting enzyme inhibitors; ARB: angiotensin receptor blockers; BMS: bare metal stent; CABG: coronary artery bypass graft; DES: drug eluting stent; eGFR: estimated glomerular filtration rate; HbA1c: hemoglobin A1c; IQR: interquartile range; LVEF: left ventricular ejection fraction; NSTEMI: non-ST-segment elevation myocardial infarction; PCI: percutaneous coronary intervention; PTCA: percutaneous transluminal coronary angioplasty; UA: unstable angina.
As to in-hospital outcomes, there was no difference between patients with HbA1c < 7% and patients with HbA1c ≥ 7% in all-cause death, MACEs and any bleeding, but those whose HbA1c ≥ 7% had higher incidence of major bleeding. (1.5% vs. 2.3%, P = 0.038; Table 2). After adjusted by multivariable models, baseline HbA1c levels ≥7% did not show association with a higher risk of major bleeding (adjusted OR: 1.40, 95% CI: 0.81-2.44, P = 0.230), all-cause death (adjusted OR: 0.19, 95% CI: 0.02-1.49, P = 0.114), MACEs (adjusted OR: 0.87, 95% CI: 0.44-1.74, P = 0.703), and any bleeding (adjusted OR: 0.86, 95% CI: 0.68-1.09, P = 0.218; Table 2 and Table 4).
Table
2.
In-hospital clinical outcomes according to HbA1c levels.
Outcome
HbA1c ≥ 7% (n = 1543)
HbA1c < 7% (n = 4740)
Total (n = 6283)
P-value
All-cause death
1 (0.1%)
11 (0.2%)
12 (0.2%)
0.191
MACEs
11 (0.7%)
35 (0.7%)
46 (0.7%)
0.919
TVR
0
4 (0.1%)
4 (0.1%)
0.254
Ischemic stroke
5 (0.3%)
7 (0.1%)
12 (0.2%)
0.168
Myocardial infarction
5 (0.3%)
18 (0.4%)
23 (0.4%)
0.753
Major bleeding
36 (2.3%)
73 (1.5%)
109 (1.7%)
0.038
Any bleeding
191 (12.4%)
627 (13.2%)
818 (13.0%)
0.389
Data are presented as n (%). HbA1c: Hemoglobin A1c; MACEs: major adverse cardiovascular events; TVR: target vessel revascularization.
Table
4.
Univariate and multivariable logistic regression and COX proportional hazards regression for the association of baseline HbA1c levels with outcomes.
Compared with the patients with HbA1c < 7%, the risk of major bleeding events was higher in the patients with HbA1c ≥ 7% during long-term follow-up but not in short-term follow-up (in 30 days: adjusted HR = 1.48; 95% CI: 0.86-2.55; P = 0.153, in the whole follow-up: adjusted HR = 1.57; 95% CI: 1.01-2.44; P = 0.044; Table 3 and Table 4). No difference was observed in all-cause death and any bleeding between the patients with HbA1c < 7% and with HbA1c ≥ 7% (all-cause death: adjusted HR = 0.88; 95% CI: 0.66-1.18; P = 0.398; any bleeding: adjusted HR = 1.00, 95% CI: 0.84-1.19, P = 0.994; Table 3 and Table 4). After adjustment of potential confounders included in multivariable analyses, Cox regression plots showed that the patients with HbA1c ≥ 7% had more major bleeding events (P = 0.044), whereas the all-cause death occurred similarly in both patients with HbA1c ≥ 7% and with HbA1c < 7% (P = 0.398; Figure S1 in supplemental materials). As to the Kaplan-Meier analyses for major bleeding, more major bleeding occurred in patients with HbA1c ≥ 7% in the first 30 days, from 30 days to 6 years and the whole duration of follow-up (P = 0.027, P = 0.049, P = 0.003, respectively; Figure 2). The long-term mortality was lower in those patients with HbA1c < 7% (P = 0.005; Figure 2).
Figure
2.
Kaplan-Meier estimated event rates of major bleeding and all-cause death according to baseline HbA1c levels.
Solid lines indicate the Kaplan-Meier curves, and the shaded area is the 95% CI. HbA1c: Hemoglobin A1c.
Generally, the association between baseline glycemic status on admission and major bleeding was consistent across subgroups with primary analyses. There was no significant interaction between baseline HbA1c levels and other baseline characteristics factors, including the previous diagnosis of T2DM and chronic kidney disease (P for interaction > 0.10 in all comparisons; Figure 3). Also, no significant interaction between baseline HbA1c levels and insulin use or other hypoglycemic treatment use (P for interaction = 0.177 and = 0.674, respectively; Figure S2 in supplemental materials).
Figure
3.
Subgroup analyses for the association between baseline hba1c and major bleeding.
This study aimed to investigate the association between baseline HbA1c levels and bleeding in NSTE-ACS patients undergoing PCI. We found that compared with baseline HbA1c < 7%, baseline HbA1c levels ≥ 7% were associated with a higher long-term risk of major bleeding but not associated with all-cause death in patients with NSTE-ACS undergoing PCI.
Compared with NSTE-ACS patients who received conservative strategies, the patients undergoing PCI who were administered additional anticoagulants during the procedure had a higher risk of bleeding events.[11,12] Although DM was reported as a risk factor both for ischemic events and bleeding in NSTEMI patients,[5] limited studies have investigated the association between DM and bleeding events in NSTE-ACS patients undergoing PCI.
There are inconsistent observations in the association between HbA1c levels with all-cause death. The previous studies showed that baseline HbA1c was an independent predictive factor for all-cause death regardless of whether the patients had a previous diagnosis of DM.[10,15,16] Recently, Baber, et al.[9] reported that in patients with ACS undergoing PCI, baseline HbA1c levels display a U-shaped association with long-term all-cause death or myocardial infarction, where the lower HbA1c levels were also related to a higher ischemic event. Engoren, et al.[17] also reported that patients with lower HbA1c undergoing CABG had more cardiovascular death events.
In the present study, the crude K-M curve showed that relative to baseline HbA1c < 7%, baseline HbA1c levels ≥ 7% were associated with more all-cause death events. After adjustment with several potential confounders, there was no significance in the association between HbA1c levels and all-cause death, which possibly suggested that several confounders raised from higher HbA1c levels may be adjusted in this study.
Diabetes was identified as associated with major bleeding events, including gastrointestinal bleeding and intracranial bleeding.[18] The Can Rapid risk stratification of Unstable angina patients Suppress ADverse outcomes with Early implementation of the ACC/AHA guidelines (CRUSADE) bleeding score enrolled the history of diabetes as an independent predictive factor for post-MI bleeding risk.[5]
The current evidence showed inconsistent results. Consistent with the CRUSADE study, Giraldez, et al.[15] found that in patients with NSTE-ACS, compared with those who had normal glycemic status, those who had DM experienced a higher risk of bleeding events defined by GUSTO moderate or severe bleeding. On the contrary, several recent studies failed to confirm the roles of DM in increasing the risk of bleeding in patients with coronary artery diseases undergoing PCI.[19-22] Given that HbA1c levels were considered a better reflection of the glycemic status of patients than instant blood glucose or the history of DM, it might play a more crucial role in maintaining the balance between ischemia and bleeding.[23] In the latest study, Samuelsen, et al.[24] reported DM defined by HbA1c was identified as the risk factor for the higher risk of major bleeding in patients undergoing PCI. Additionally, a previous study conducted on patients with stable coronary diseases reported that the higher baseline HbA1c was also associated with a higher incidence of major bleeding (BARC > 2 grade) in patients.[25] The subgroup analysis of the PLATO study also showed that the higher HbA1c was associated with a higher incidence of bleeding events in ACS patients receiving invasive or non-invasive strategies. However, there was limited evidence to investigate the association of HbA1c with bleeding events in NSTE-ACS patients undergoing PCI.
In this study, we found that the NSTE-ACS patients with higher baseline HbA1c levels undergoing PCI had more incidences of major bleeding (3-5 grade). The reasons why high HbA1c levels are associated with bleeding remain unclear. Lemesle et al. thought physicians would tend to provide more stringent secondary prevention to DM patients for reducing the incidence of ischemic events. Still, these strategies may increase the risk of bleeding in turn.[25] Additionally, the patients who were enrolled in the CORONOR study and EARLY ACS study where the higher HbA1c levels or DM were associated with higher bleeding risk, might be more administrated aspirin and clopidogrel.[15,25] The previous study suggested that clopidogrel usage may increase the risk of bleeding in patients with DM.[22,24] There also were a high proportion of aspirin use and clopidogrel use in our study (aspirin: 100.0% and clopidogrel: 99.1%), which may enhance the potential effect of HbA1c on bleeding in patients with NSTE-ACS undergoing PCI, but the clear mechanism should be further elucidated.
Moreover, we noticed that new major bleeding events burst in the first 30 days and the accumulation trend flatten from 30 days to 6-year follow-up. This trend may suggest the impact of HbA1c levels on bleeding events throughout in-hospital antithrombotic medication and discharge antiplatelet management in general. Also, the glucose-lowering drugs, including metformin and sulfonylureas, may interact with antithrombotic therapies to decrease platelet activity, which may be the underlying reason for a higher incidence of bleeding events in this study.[26] Another potential mechanism could be attributed to the higher PAI-1 and t-PA levels indicating a disorder in the fibrinolytic system in DM patients.[27] Hyperglycemia status and increased insulin levels can stimulate the production of PAI-1 by endothelial cells and adipocytes.[28-31] The increase in PAI-1 reduces the serine protease effect of rtPA, which may produce increased endothelial damage, blood-brain barrier breakdown, and microvasculature, leading to hemorrhagic complications.[32,33] However, clearer mechanisms of the relation between glycemic status and bleeding still should be further studied.
Although the previous studies found that the administration of insulin increased the incidence of mortality,[34] this was not associated with the higher risk of bleeding events in patients with ACS.[19] Consistently, in the present study, the subgroup analyses failed to find the differences in the association between the risk of bleeding and HbA1c levels in the patients with or without insulin or hypoglycemic treatments. These indicated that further studies are required for investigating the association between insulin or hypoglycemic treatments and bleeding in patients with NSTE-ACS undergoing PCI.
LIMITATIONS
First, this study is an observational cohort study, meaning several potential confounders impacted the results. We minimized this impact by enrolling multivariate analyses, but there still are residual confounders unadjusted. Second, the low incidence of events makes subgroup analyses insufficient to find the predictive effect of baseline HbA1c levels in patients with DM or without DM. Alternatively, further studies could enroll the NSTE-ACS patients with or without DM respectively to demonstrate the roles of baseline HbA1c in the prediction of bleeding events in a different group. Third, this study didn’t record the HbA1c levels during follow-up or long-term glucose-lowering strategies. Therefore, it could not determine the long-term glycemic status on clinical outcomes in patients undergoing PCI for NSTE-ACS.
CONCLUSION
Compared with the lower baseline HbA1c levels, the higher baseline HbA1c levels were associated with an increase in long-term bleeding risk in NSTE-ACS patients undergoing PCI, though higher baseline HbA1c levels were not associated with a higher risk of mortality.
ETHICS
The study protocol was approved by the central ethics committee of the Guangdong Provincial People’s Hospital, Guangzhou, China, with a waiver of informed consent (No. GDREC2016210H(R1)).
FUNDINGS
This work was supported by Outstanding Young Medical Talents in Guangdong Province (KJ012019456), the Outstanding Young Talent Program of Guangdong Provincial People’s Hospital (Grant No. KJ012019084 and KJ012019095), the High-level Hospital Construction Project (Grant No. DFJH2020021), Guangdong Provincial People’s Hospital Clinical Research Fund (Y012018085), and National Natural Science Foundation of Guangdong Province (KC022021005).
Roffi M, Patrono C, Collet JP, et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur Heart J 2016; 37: 267−315. doi: 10.1093/eurheartj/ehv320
[2]
Donahoe SM, Stewart GC, McCabe CH, et al. Diabetes and mortality following acute coronary syndromes. JAMA 2007; 298: 765−775. doi: 10.1001/jama.298.7.765
[3]
Dotevall A, Hasdai D, Wallentin L, et al. Diabetes mellitus: clinical presentation and outcome in men and women with acute coronary syndromes. Data from the Euro Heart Survey ACS. Diabet Med 2005; 22: 1542−1550.
[4]
Godoy LC, Lawler PR, Farkouh ME, et al. Urgent revascularization strategies in patients with diabetes mellitus and acute coronary syndrome. Can J Cardiol 2019; 35: 993−1001. doi: 10.1016/j.cjca.2019.03.010
[5]
Subherwal S, Bach RG, Chen AY, et al. Baseline risk of major bleeding in non-ST-segment-elevation myocardial infarction: the CRUSADE (Can Rapid risk stratification of Unstable angina patients Suppress ADverse outcomes with Early implementation of the ACC/AHA Guidelines) Bleeding Score. Circulation 2009; 119: 1873−1882. doi: 10.1161/CIRCULATIONAHA.108.828541
[6]
Liu R, Lyu SZ, Zhao GQ, et al. Comparison of the performance of the CRUSADE, ACUITY-HORIZONS, and ACTION bleeding scores in ACS patients undergoing PCI: insights from a cohort of 4939 patients in China. J Geriatr Cardiol 2017; 14: 93−99.
[7]
Cosentino F, Grant PJ, Aboyans V, et al. 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur Heart J 2020; 41: 255−323. doi: 10.1093/eurheartj/ehz486
[8]
Neumann FJ, Sousa-Uva M, Ahlsson A, et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur Heart J 2019; 40: 87−165. doi: 10.1093/eurheartj/ehy394
[9]
Baber U, Azzalini L, Masoomi R, et al. Hemoglobin A1c and cardiovascular outcomes following percutaneous coronary intervention: insights from a large single-center registry. JACC Cardiovasc Interv 2021; 14: 388−397. doi: 10.1016/j.jcin.2020.10.008
[10]
James S, Angiolillo DJ, Cornel JH, et al. Ticagrelor vs. clopidogrel in patients with acute coronary syndromes and diabetes:a substudy from the PLATelet inhibition and patient Outcomes (PLATO) trial. Eur Heart J 2010; 31: 3006−3016.
[11]
Lopes RD, Subherwal S, Holmes DN, et al. The association of in-hospital major bleeding with short-, intermediate-, and long-term mortality among older patients with non-ST-segment elevation myocardial infarction. Eur Heart J 2012; 33: 2044−2053. doi: 10.1093/eurheartj/ehs012
[12]
Hoenig MR, Doust JA, Aroney CN, Scott IA. Early invasive versus conservative strategies for unstable angina & non-ST-elevation myocardial infarction in the stent era. Cochrane Database Syst Rev 2006: CD004815.
[13]
Chen JY, He PC, Liu YH, et al. Association of parenteral anticoagulation therapy with outcomes in chinese patients undergoing percutaneous coronary intervention for non–ST-segment elevation acute coronary syndrome. JAMA Internal Medicine 2019; 179: 186. doi: 10.1001/jamainternmed.2018.5953
[14]
Mehran R, Rao SV, Bhatt DL, et al. Standardized bleeding definitions for cardiovascular clinical trials: a consensus report from the Bleeding Academic Research Consortium. Circulation 2011; 123: 2736−747. doi: 10.1161/CIRCULATIONAHA.110.009449
[15]
Giraldez RR, Clare RM, Lopes RD, et al. Prevalence and clinical outcomes of undiagnosed diabetes mellitus and prediabetes among patients with high-risk non-ST-segment elevation acute coronary syndrome. Am Heart J 2013; 165: 918−25 e2.
[16]
Timmer JR, Hoekstra M, Nijsten MW, et al. Prognostic value of admission glycosylated hemoglobin and glucose in nondiabetic patients with ST-segment-elevation myocardial infarction treated with percutaneous coronary intervention. Circulation 2011; 124: 704−711. doi: 10.1161/CIRCULATIONAHA.110.985911
[17]
Engoren M, Schwann TA, Arslanian-Engoren C, et al. U-shape association between hemoglobin A1c and late mortality in patients with heart failure after cardiac surgery. Am J Cardiol 2013; 111: 1209−1213. doi: 10.1016/j.amjcard.2012.12.054
[18]
De Berardis G, Lucisano G, D'Ettorre A, et al. Association of aspirin use with major bleeding in patients with and without diabetes. JAMA 2012; 307: 2286−2294.
[19]
Chichareon P, Modolo R, Kogame N, et al. Association of diabetes with outcomes in patients undergoing contemporary percutaneous coronary intervention: Pre-specified subgroup analysis from the randomized GLOBAL LEADERS study. Atherosclerosis 2020; 295: 45−53. doi: 10.1016/j.atherosclerosis.2020.01.002
[20]
Ploumen EH, Pinxterhuis TH, Zocca P, et al. Impact of prediabetes and diabetes on 3-year outcome of patients treated with new-generation drug-eluting stents in two large-scale randomized clinical trials. Cardiovasc Diabetol 2021; 20: 217. doi: 10.1186/s12933-021-01405-4
[21]
Cavallari I, Maddaloni E, Gragnano F, et al. Ischemic and bleeding risk by type 2 diabetes clusters in patients with acute coronary syndrome. Intern Emerg Med 2021; 16: 1583−1591. doi: 10.1007/s11739-021-02640-z
[22]
Simek S, Motovska Z, Hlinomaz O, et al. The effect of diabetes on prognosis following myocardial infarction treated with primary angioplasty and potent antiplatelet therapy. J Clin Med 2020; 9: 2555. doi: 10.3390/jcm9082555
[23]
Selvin E, Steffes MW, Zhu H, et al. Glycated hemoglobin, diabetes, and cardiovascular risk in nondiabetic adults. N Engl J Med 2010; 362: 800−811. doi: 10.1056/NEJMoa0908359
[24]
Samuelsen PJ, Eggen AE, Steigen T, et al. Incidence and risk factors for major bleeding among patients undergoing percutaneous coronary intervention: Findings from the Norwegian Coronary Stent Trial (NORSTENT). PLoS One 2021; 16: e0247358. doi: 10.1371/journal.pone.0247358
[25]
Lemesle G, Meurice T, Tricot O, et al. Association of diabetic status and glycemic control with ischemic and bleeding outcomes in patients with stable coronary artery disease: The 5-Year CORONOR Registry. J Am Heart Assoc 2018; 7: e008354. doi: 10.1161/JAHA.117.008354
[26]
Nusca A, Tuccinardi D, Pieralice S, et al. Platelet effects of anti-diabetic therapies: new perspectives in the management of patients with diabetes and cardiovascular disease. Front Pharmacol 2021; 12: 670155. doi: 10.3389/fphar.2021.670155
[27]
Meigs JB, Mittleman MA, Nathan DM, et al. Hyperinsulinemia, hyperglycemia, and impaired hemostasis: the Framingham Offspring Study. JAMA 2000; 283: 221−228. doi: 10.1001/jama.283.2.221
[28]
Pandolfi A, Iacoviello L, Capani F, et al. Glucose and insulin independently reduce the fibrinolytic potential of human vascular smooth muscle cells in culture. Diabetologia 1996; 39: 1425−1431. doi: 10.1007/s001250050594
[29]
Morange PE, Aubert J, Peiretti F, et al. Glucocorticoids and insulin promote plasminogen activator inhibitor 1 production by human adipose tissue. Diabetes 1999; 48: 890−895. doi: 10.2337/diabetes.48.4.890
[30]
Alessi MC, Peiretti F, Morange P, et al. Production of plasminogen activator inhibitor 1 by human adipose tissue: possible link between visceral fat accumulation and vascular disease. Diabetes 1997; 46: 860−867. doi: 10.2337/diab.46.5.860
[31]
Nordt TK, Klassen KJ, Schneider DJ, Sobel BE. Augmentation of synthesis of plasminogen activator inhibitor type-1 in arterial endothelial cells by glucose and its implications for local fibrinolysis. Arterioscler Thromb 1993; 13: 1822−1828. doi: 10.1161/01.ATV.13.12.1822
[32]
Shatos MA, Doherty JM, Penar PL, Sobel BE. Suppression of plasminogen activator inhibitor-1 release from human cerebral endothelium by plasminogen activators. A factor potentially predisposing to intracranial bleeding. Circulation 1996; 94: 636−642.
Sharma PK, Agarwal S, Ellis SG, et al. Association of glycemic control with mortality in patients with diabetes mellitus undergoing percutaneous coronary intervention. Circ Cardiovasc Interv 2014; 7: 503−509. doi: 10.1161/CIRCINTERVENTIONS.113.001107
Wang M, Su W, Chen H, et al. The joint association of diabetes status and NT-ProBNP with adverse cardiac outcomes in patients with non-ST-segment elevation acute coronary syndrome: a prospective cohort study. Cardiovasc Diabetol, 2023, 22(1): 46.
DOI:10.1186/s12933-023-01771-1
Table
4.
Univariate and multivariable logistic regression and COX proportional hazards regression for the association of baseline HbA1c levels with outcomes.


 DownLoad:
DownLoad:


