Please cite this article as: Kurihara O, Takano M, Shibata Y, Kobayashi N, Miyauchi Y, Asai K. Are angiographic culprit lesions true? Disagreement between angiographic and optical coherence tomographic detection. J Geriatr Cardiol 2021; 18(10): 844−846. DOI: 10.11909/j.issn.1671-5411.2021.10.010.
Citation:
Please cite this article as: Kurihara O, Takano M, Shibata Y, Kobayashi N, Miyauchi Y, Asai K. Are angiographic culprit lesions true? Disagreement between angiographic and optical coherence tomographic detection. J Geriatr Cardiol 2021; 18(10): 844−846. DOI: 10.11909/j.issn.1671-5411.2021.10.010.
Please cite this article as: Kurihara O, Takano M, Shibata Y, Kobayashi N, Miyauchi Y, Asai K. Are angiographic culprit lesions true? Disagreement between angiographic and optical coherence tomographic detection. J Geriatr Cardiol 2021; 18(10): 844−846. DOI: 10.11909/j.issn.1671-5411.2021.10.010.
Citation:
Please cite this article as: Kurihara O, Takano M, Shibata Y, Kobayashi N, Miyauchi Y, Asai K. Are angiographic culprit lesions true? Disagreement between angiographic and optical coherence tomographic detection. J Geriatr Cardiol 2021; 18(10): 844−846. DOI: 10.11909/j.issn.1671-5411.2021.10.010.
Coronary angiography provides a two-dimensional silhouette of the vascular lumen. It is the gold standard for the diagnosis of coronary artery disease and is essential during percutaneous coronary intervention (PCI). Intravascular optical coherence tomography (OCT) with high-resolution images enables direct visualization of the microscopic features of a plaque, including its fibrous cap, micro-vessels, thrombus, inflammatory cells, and cholesterol crystals[1,2] and has recently been used during PCI procedures; there is growing evidence that OCT-guided PCI has potential benefits regarding optimal stenting.[3,4] Based on coronary angiography findings, OCT observation is performed to calculate and/or evaluate the diameter and/or characteristics of angiographic culprit lesions, following which PCI procedures are performed. Conversely, our series of acute myocardial infarction (AMI) showed that angiographic culprit lesions were quite far from the culprit plaques identified using OCT.
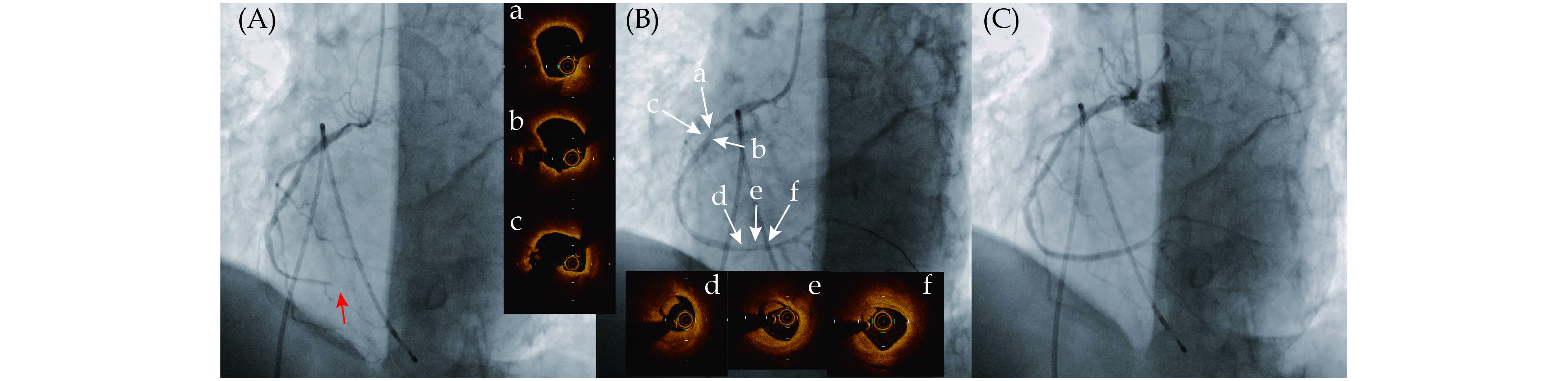
Case 1. An 87-year-old man patient had ST-segment elevation myocardial infarction (STEMI). Initial coronary angiography showed total occlusion of the distal right coronary artery (RCA), which was suspected to be the culprit lesion (Figure 1A). After a balloon angioplasty for the distal RCA lesion, coronary angiography and OCT observation were performed from the distal RCA to the proximal RCA (Figure 1B). OCT shows a disrupted thin-cap fibroatheroma (TCFA) with a thrombus in a region within the proximal RCA that showed mild stenosis on angiography. This lesion was the true culprit according to the OCT findings (Figure 1Ba-1Bc). In the distal RCA, which was suspected to harbor the culprit lesion on angiography, OCT showed luminal narrowing and residual thrombus (Figure 1Bd-1Bf). Final coronary angiography showed a dilated lumen with no limitations to blood flow (Figure 1C).
Figure
1.
An 87-year-old male patient with ST-segment elevation myocardial infarction: angiography shows total occlusion in the distal RCA, while the OCT-derived culprit lesion is in the proximal RCA.
(A): Baseline coronary angiography shows total occlusion of the distal RCA (red arrow), suspected to be the culprit lesion; (B): after balloon angioplasty for the distal RCA lesion, the distal to the proximal RCA were evaluated by coronary angiography and OCT; OCT shows a disrupted thin-cap fibroatheroma with a thrombus in a region within the proximal RCA that showed mild stenosis on angiogram. This was the true culprit lesion according to OCT (a–c), OCT shows luminal narrowing and residual thrombus in the distal RCA (d–f); and (C): after percutaneous coronary intervention, coronary angiography showed a dilated lumen without flow limitations. OCT: optical coherence tomography; RCA: right coronary artery.
Case 2. A 54-year-old male patient had STEMI. Initial coronary angiography showed total occlusion of the second diagonal branch and severe stenosis in the mid left anterior descending artery (LAD) (Figure 2A). After balloon angioplasty for a suspected culprit lesion in the second diagonal branch, coronary angiography and OCT were performed from the mid LAD to the proximal LAD (Figure 2B). Surprisingly, a disrupted TCFA and a thrombus were observed using OCT in the region of an angiographically mild stenosis of the proximal LAD (Figure 2Ba-2Bc). OCT showed that the thrombi were attached to the vessel wall and there was no disrupted plaque at the severely stenosed region in the mid LAD (Figure 2Bd-2Bf). Shower emboli from the proximal LAD lesion occluded the second diagonal branch and narrowed the lumen of the mid LAD. Final results of angiography were excellent and showed thrombolysis in myocardial infarction (TIMI) grade 3 coronary flow (Figure 2C).
Figure
2.
A 54-year-old male patient with ST-segment elevation myocardial infarction: angiography shows total occlusion of the second diagonal branch, while the OCT-derived culprit lesion is in the proximal LAD.
(A): Baseline coronary angiography shows total occlusion of the second diagonal branch and severe stenosis in the mid LAD (red arrows); (B): after balloon angioplasty for a suspected culprit lesion in the second diagonal branch, coronary angiography and OCT were performed from the mid LAD to the proximal LAD (white arrows). OCT revealed a disrupted thin-cap fibroatheroma and a thrombus in the region of an angiographically mild stenosis of the proximal LAD (a–c), OCT shows that the thrombi were attached to the vessel wall and there was no disrupted plaque at the severely stenosed region in the mid LAD. Shower emboli from the proximal LAD lesion occluded the second diagonal branch and narrowed the lumen of the mid LAD (d–f); and (C): final results of angiography were excellent with thrombolysis in myocardial infarction grade 3 coronary flow. LAD: left anterior descending artery; OCT: optical coherence tomography.
Case 3. A 70-year-old man patient had STEMI. Initial coronary angiography showed a sub-total occlusion of the distal left circumflex artery (LCx) (Figure 3A). After balloon angioplasty for the distal LCx, coronary angiography and OCT were performed from the distal LCx to the mid LCx (Figure 3B). OCT showed disrupted intima at a region of mild stenosis in the mid LCx (Figure 3Ba-3Bc). OCT showed that the lumen was narrowed due to thrombi, these thrombi are the angiographic culprits in the distal LCx (Figure 3Bd-3Bf). Final coronary angiography showed a dilated lumen and TIMI grade 3 flow (Figure 3C).
Figure
3.
A 70-year-old male patient with ST-segment elevation myocardial infarction: sub-total occlusion in the distal LCx, while the OCT-derived culprit lesion is in the mid LCx.
(A): Baseline coronary angiography shows a sub-total occlusion of the distal LCx (red arrow); (B): after balloon angioplasty for the distal LCx, coronary angiography and OCT were performed from the distal to the mid LCx (white arrows). OCT shows a disrupted intima at a region of mild stenosis in the mid LCx (a–c), OCT shows narrowed lumen due to thrombi; these thrombi are the angiographic culprits in the distal LCx (d–f); and (C): after percutaneous coronary intervention, coronary angiography shows a dilated lumen and thrombolysis in myocardial infarction grade 3 flow. LCx: left circumflex artery; OCT: optical coherence tomography.
Generally, thrombus formation on the disrupted plaque occludes the coronary lumen and leads to AMI.[5] It is believed that the angiographic narrowest or occluded site is the culprit lesion; however, our cases showed discrepancies in the location of the culprit lesions between angiography and OCT. There is a new concept of myocardial infarction with nonobstructive coronary arteries (MINOCA), which is defined as myocardial infarction without angiographically moderate to severe stenosis (> 50%).[6] Plaque disruption and thrombi have been found through OCT observation in 24% and 18%, respectively, of patients with MINOCA,[7] and thrombi on disrupted plaque without significant stenosis on coronary angiography induce myocardial injury. In our cases, OCT findings of angiographic culprit lesions at the narrowest lumen showed that thrombi were attached to the vessel wall with no evidence of plaque disruption. In addition, disrupted TCFA was observed at mild stenosis proximal to the narrowest lesion. If significant stenosis were located distally to the proximal disrupted culprit plaque, embolization occurring distal to the true culprit lesion may occasionally create a deceptive culprit lesion on coronary angiography. OCT observation of the whole vessel, especially proximal to the suspected culprit lesion, may be valuable for the detection of the true culprit lesion and the following optimal intervention.
We revealed disagreement in the site of the culprit plaque between angiography and OCT. In cases of AMI, OCT observation of the whole culprit vessel enables precise detection of culprit lesions.
ACKNOWLEDGMENTS
All authors had no conflicts of interest to disclose.
Jang IK, Bouma BE, Kang DH, et al. Visualization of coronary atherosclerotic plaques in patients using optical coherence tomography: comparison with intravascular ultrasound. J Am Coll Cardiol 2002; 39: 604−609. doi: 10.1016/S0735-1097(01)01799-5
[2]
Tearney GJ, Regar E, Akasaka T, et al. Consensus standards for acquisition, measurement, and reporting of intravascular optical coherence tomography studies: a report from the International Working Group for Intravascular Optical Coherence Tomography Standardization and Validation. J Am Coll Cardiol 2012; 59: 1058−1072. doi: 10.1016/j.jacc.2011.09.079
[3]
Jones DA, Rathod KS, Koganti S, et al. Angiography alone versus angiography plus optical coherence tomography to guide percutaneous coronary intervention: outcomes from the Pan-London PCI cohort. JACC Cardiovasc Interv 2018; 11: 1313−1321. doi: 10.1016/j.jcin.2018.01.274
[4]
Räber L, Mintz GS, Koskinas KC, et al. Clinical use of intracoronary imaging. Part 1: guidance and optimization of coronary interventions. An expert consensus document of the European Association of Percutaneous Cardiovascular Interventions. Eur Heart J 2018; 39: 3281−3300. doi: 10.1093/eurheartj/ehy285
[5]
Fuster V, Badimon L, Badimon JJ, et al. The pathogenesis of coronary artery disease and the acute coronary syndromes (1). N Engl J Med 1992; 326: 242−250. doi: 10.1056/NEJM199201233260406
[6]
Collet JP, Thiele H, Barbato E, et al. 2020 ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J 2021; 42: 1289−1367. doi: 10.1093/eurheartj/ehaa575
[7]
Opolski MP, Spiewak M, Marczak M, et al. Mechanisms of myocardial infarction in patients with nonobstructive coronary artery disease: results from the Optical Coherence Tomography Study. JACC Cardiovasc Imaging 2019; 12: 2210−2221. doi: 10.1016/j.jcmg.2018.08.022


 DownLoad:
DownLoad:


